Medical Expense Insurance
Historically, health insurance was designed to shield individuals from routine, predictable costs—a few days in a hospital bed or a standard procedure. These early models functioned like prepaid maintenance plans, offering immediate relief for minor expenses but collapsing under the weight of severe illness. As medical technology advanced and costs multiplied, the industry was forced into a radical architectural shift: from basic, fragmented policies that paid fixed sums, to comprehensive managed care systems designed to cap financial ruin. For an insurance producer, mastering this evolution is not a history lesson; it is the fundamental blueprint for understanding every modern policy structure you will analyze, recommend, or explain to a client.
To understand modern health insurance, you must first understand the system it replaced. Basic medical expense insurance was the original standard. The defining characteristic of these plans is that they provide first-dollar coverage.
First-Dollar Coverage: The insurer begins paying benefits immediately upon the occurrence of a covered claim. Basic medical expense policies do not require the insured to pay a deductible before benefits are paid.
Because the insurer takes on the risk from the very first dollar, these plans must rigorously limit their exposure. Consequently, basic medical expense policies generally have low benefit limits compared to major medical plans.
Instead of a single pool of money, basic medical expense insurance typically divides coverage into separate, isolated categories: hospital, surgical, and medical.
Basic Hospital Expense Coverage
If your client is admitted to the hospital, basic hospital expense coverage pays for room and board during a hospital stay. However, it does not pay a blank check. The policy often provides a specific dollar benefit amount per day for room and board (e.g., $200 per day for up to 30 days). If the actual hospital room costs $500 a day, the client pays the $300 difference out-of-pocket.
Basic Surgical Expense Coverage
This category covers the operating room. Basic surgical expense coverage can pay surgeons' fees using one of two distinct mathematical approaches:
- A surgical schedule: This is a literal list inside the policy. A surgical schedule assigns a specific dollar value to each surgical procedure. (e.g., Appendectomy = $1,500).
- A relative value scale: Instead of listing dollar amounts, a relative value scale assigns a point value to a surgical procedure to calculate the benefit amount. A complex surgery might be assigned 100 points, while a minor one is assigned 10 points. A conversion factor (e.g., $20 per point) is then multiplied by the points to determine the payout.
Basic Physicians' Nonsurgical Expense Coverage
If a physician visits a patient in the hospital for observation or treatment that does not involve a scalpel, the surgical policy will not cover it. Instead, basic physicians' nonsurgical expense coverage pays for doctor visits while the insured is hospitalized.
Basic plans left patients disastrously exposed if they contracted a severe illness like cancer or required a prolonged ICU stay. The industry's solution was Major medical expense insurance, which is designed to protect policyholders against catastrophic medical expenses.

Because these plans are built for disaster rather than routine maintenance, major medical insurance policies feature high maximum benefit limits—often stretching into the millions. But to afford offering such high limits, the insurer requires the policyholder to share the initial risk. Major medical insurance policies require the insured to satisfy a deductible before benefits are paid.
The Mathematics of Major Medical
Major medical plans follow a strict, sequential mathematical formula for claims. As a producer, you must be able to walk your client through these three steps:
Step 1: The Flat Deductible Before the insurer pays a dime, the insured must pay a flat deductible, which is a stated dollar amount the insured must pay out-of-pocket before major medical benefits begin. (e.g., $1,000).
Step 2: Coinsurance Once the deductible is met, the insurer does not immediately take over 100% of the bill. Instead, major medical insurance policies utilize coinsurance to share costs between the insurer and the insured.
Coinsurance is the specific percentage of covered medical expenses shared between the insurer and the insured after the deductible is met.
A common coinsurance provision requires the insurer to pay 80 percent of covered medical expenses, while the insured is required to pay 20 percent.
Step 3: The Stop-Loss Provision If a patient has an $800,000 hospital bill, a 20% coinsurance requirement would still bankrupt them ($160,000). To prevent this, major medical policies include a cap. A stop-loss provision limits the total out-of-pocket expenses an insured must pay in a single calendar year. Because it caps the client's financial bleeding, the stop-loss provision is frequently referred to as the out-of-pocket maximum.
Crucially, once the stop-loss limit is reached, the insurer pays 100 percent of covered expenses for the remainder of the year.
A Worked Example
Your client suffers a heart attack resulting in a $51,000 medical bill. They have a major medical policy with a $1,000 flat deductible, 80/20 coinsurance, and a $5,000 stop-loss (out-of-pocket maximum).
- Deductible: The client pays the first $1,000. (Remaining bill: $50,000. Client out-of-pocket so far: $1,000)
- Coinsurance: The remaining $50,000 is split 80/20. The client owes 20%, which is $10,000.
- Stop-Loss Intervention: The client's total out-of-pocket costs are capped at $5,000 for the year. Since they already paid the $1,000 deductible, they will only pay $4,000 of that $10,000 coinsurance bill.
- Result: The client pays exactly $5,000. The insurer pays the remaining $46,000. For the rest of the calendar year, the insurer will pay 100% of covered medical bills.
Eventually, insurers realized that forcing clients to buy a basic policy for minor issues and a major medical policy for severe issues was inefficient. The solution was Comprehensive major medical insurance, which combines basic medical expense coverage and major medical coverage into a single policy.
Here is the architectural trick: How do you connect a first-dollar basic plan to a major medical plan? You use a corridor.
In these policies, the basic portion pays first. Once the basic benefits are exhausted, the client must pay out-of-pocket before the catastrophic coverage kicks in. This gap is known as a corridor deductible. Just as a physical corridor connects two separate rooms, the corridor deductible bridges the gap between the exhaustion of basic medical benefits and the start of major medical benefits.
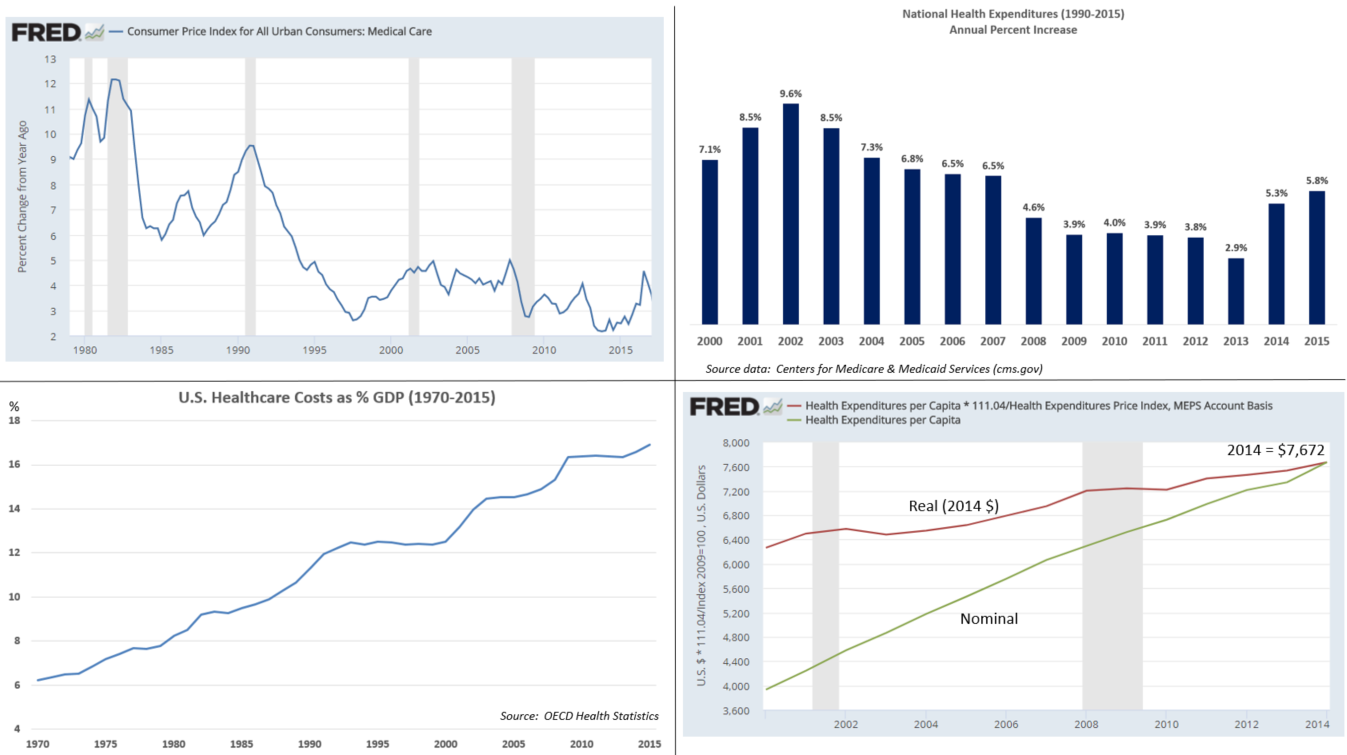
Traditional major medical plans essentially told doctors: "Cure the patient, send us the bill." This caused healthcare costs to skyrocket. Insurers realized that to control costs, they couldn't just pay the bills; they had to manage the care itself.
Health Maintenance Organizations (HMOs)
A Health Maintenance Organization provides both the financing of healthcare and the delivery of patient care for its members. Unlike traditional insurers that just write checks, an HMO essentially acts as both the insurance company and the hospital network.
To keep costs down, the HMO model relies on several strict structural pillars:
- Preventive Care: It is cheaper to treat high blood pressure today than to pay for open-heart surgery tomorrow. Therefore, an HMO heavily emphasizes preventive care to reduce long-term healthcare costs. Because of this, HMOs typically cover routine physical exams and well-child care.
- The Gatekeeper System: To prevent patients from unnecessarily booking expensive specialists, HMO members are generally required to choose a Primary Care Physician (PCP). This PCP acts as a gatekeeper for all medical care. If a member's knee hurts, they cannot go straight to an orthopedic surgeon; the member must obtain a referral from the PCP to see a medical specialist.
- Geographic and Network Strictness: An HMO requires members to live within a specified geographic service area. Furthermore, to control costs, HMOs generally do not cover medical services received outside of the HMO provider network.
- The Emergency Exception: There is one universal exception to the out-of-network rule: HMOs will cover out-of-network medical services in the event of a medical emergency. (If you are having a stroke, you go to the nearest hospital, network be damned).
- Copayments: Instead of complex coinsurance math, HMO members typically pay a small flat copayment for doctor visits (e.g., $20 per visit).

The Economic Engine of an HMO: Capitation How do HMOs pay their doctors? Not by the procedure. HMOs operate on a prepaid capitation basis.
Capitation: The HMO pays network providers a fixed monthly amount per member assigned to them.
Under this model, if a doctor has 1,000 HMO patients, they receive a set check every month. Capitation payments to providers remain the same regardless of how many services a member utilizes. This shifts the financial risk to the provider, incentivizing them to keep patients healthy rather than ordering unnecessary tests.
Preferred Provider Organizations (PPOs)
Many consumers hated the strict "gatekeeper" rules of HMOs. In response, the market created the PPO.
A Preferred Provider Organization contracts with a network of medical providers to offer services at discounted rates. It offers significantly more freedom than an HMO:
- No Gatekeepers: PPO members are not required to select a Primary Care Physician. Furthermore, PPO members can consult a medical specialist without obtaining a referral.
- Out-of-Network Freedom: Unlike HMOs, PPOs provide benefit coverage for both in-network and out-of-network medical services. However, this freedom comes at a cost: PPO members incur higher out-of-pocket costs when receiving care from out-of-network providers.
The Economic Engine of a PPO: Fee-for-Service Unlike the capitation model of HMOs, PPOs compensate medical providers on a fee-for-service basis.
Fee-for-Service: Medical providers are paid an agreed-upon fee for each individual service rendered to a patient.
If an in-network doctor orders an x-ray, they get paid for the x-ray. They just agree to charge the PPO's discounted rate rather than their full retail price.
HMO vs. PPO: A Quick Reference
| Feature | Health Maintenance Organization (HMO) | Preferred Provider Organization (PPO) |
|---|---|---|
| PCP Required? | Yes (Acts as Gatekeeper) | No |
| Referrals for Specialists? | Yes | No |
| Out-of-Network Coverage? | No (Except for emergencies) | Yes (But at a higher out-of-pocket cost) |
| Provider Compensation | Capitation (Prepaid fixed amount) | Fee-for-Service (Discounted rate per service) |
In insurance, whenever two extremes exist, a hybrid will inevitably emerge. A Point of Service (POS) plan combines structural features of both an HMO and a PPO.
Think of a POS plan as an HMO chassis with a PPO steering wheel. Like an HMO, the member is encouraged to select a Primary Care Physician to manage their care. However, like a PPO, the POS plan allows members to choose between an in-network or out-of-network provider each time medical care is needed.
The financial incentives dictate the client's behavior: POS plan members receive the highest level of benefits when utilizing an in-network primary care physician. If they choose to bypass the PCP and go out-of-network, they are allowed to do so, but their deductibles and coinsurance will surge dramatically. They make their choice at the "point of service."