Medicare Supplements, LTC, and Other Policies
The architecture of the United States healthcare system is a massive, interlocking grid of primary coverages that inherently leaves predictable, and sometimes financially devastating, blind spots. As an insurance professional, you will frequently sit across from clients who are entirely exposed to these blind spots—whether it is an aging client realizing Original Medicare will not cover their mounting hospital coinsurance, or a young professional caught in a coverage gap between jobs. To protect them, you must understand the specific financial instruments designed to patch these structural holes.
We will examine four foundational policies that function as specialized safety nets: Medicare Supplements (to patch the strict gaps of federal healthcare), Long-Term Care (to fund the ongoing mechanics of daily living), Accidental Death & Dismemberment (to provide sudden capital following catastrophic physical loss), and Short-Term Medical policies (to bridge temporary gaps in primary health coverage).
Original Medicare (Parts A and B) is an extraordinary federal benefit, but it is not a comprehensive shield. It operates like a robust bucket with specific, federally mandated holes: deductibles, copayments, and coinsurance. If a client experiences a severe illness, the financial leakage through those holes can bankrupt them.
To solve this, Medicare Supplement policies are also commonly known as Medigap policies. As the name suggests, Medigap policies are sold by private insurance companies to cover healthcare costs that Original Medicare does not pay.
Because Medigap is structurally tethered to Original Medicare, the eligibility rules are strict. An applicant must be enrolled in both Medicare Part A and Medicare Part B to purchase a Medigap policy. Furthermore, to prevent insurance fraud and over-insurance, Medigap policies cannot duplicate benefits already paid by Original Medicare. They only pay what Medicare leaves behind.
The Standardization of Plans
Before 1990, buying a supplement was a chaotic process for seniors, filled with confusing overlapping coverages. Today, all Medigap policies are standardized into plans labeled with letters A through N. Regardless of which private insurance company sells the policy, a Plan G from Company X provides the exact same medical benefits as a Plan G from Company Y.
At the foundation of this system is Medigap Plan A. Medigap Plan A contains the basic core benefits required by law in all Medicare Supplement policies. If an insurer wants to sell Medigap policies, they must offer Plan A.
The Core Benefits (Included in all Medigap Plans A–N) Every single Medigap policy on the market must cover these fundamental gaps:
- Part A Hospital Coinsurance: All Medigap policies must cover the Medicare Part A hospital coinsurance amount.
- Extended Hospitalization: All Medigap policies must cover hospital costs for an additional 365 days after Original Medicare benefits are exhausted.
- Part B Coinsurance/Copayments: All Medigap policies must cover the Medicare Part B coinsurance or copayment amount.
- Blood Deductible: Original Medicare does not pay for the first three pints of blood in a calendar year. Therefore, all Medigap policies must cover the cost of the first three pints of blood needed in a medical procedure each year.
- Hospice Care: All Medigap policies must cover the Medicare Part A hospice care coinsurance or copayment amount.
Consumer Protections and Enrollment
Because these policies are sold to a vulnerable, aging demographic, state and federal laws impose rigid consumer protections.
First, Medicare Supplement policies must be issued as guaranteed renewable. This is a powerful provision: an insurance company cannot cancel a Medigap policy for any reason other than the nonpayment of premiums. A client could develop terminal cancer the day after buying the policy, and the insurer must renew it. Furthermore, insurance companies must offer a 30-day free look period for all Medicare Supplement policies, allowing the senior to return the policy for a full premium refund if they change their mind.
The most critical window in your client's Medicare journey is the Open Enrollment Period. The Medigap open enrollment period lasts for six months. During this exact window, insurers cannot use medical underwriting; they must issue the policy regardless of the applicant's health.
When does the clock start? The Medigap open enrollment period begins on the first day of the month a person is both age 65 or older and enrolled in Medicare Part B. Miss this window, and your client may be subjected to medical underwriting and potentially denied coverage for pre-existing conditions.
Medical science has become incredibly adept at keeping the human body alive, but it cannot always preserve a person's independence. Original Medicare and standard health insurance are designed to cure illnesses and fix injuries. They do not pay for someone to help you get out of bed or eat your breakfast for five years.
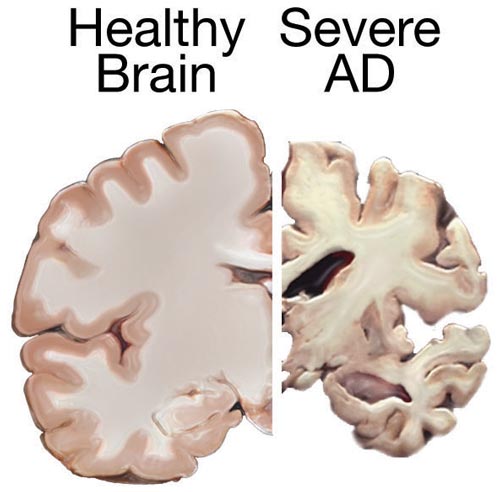
Long-Term Care insurance provides coverage for individuals who require assistance with daily living tasks due to chronic illness. Additionally, Long-Term Care insurance covers individuals who require assistance due to severe cognitive impairment, such as Alzheimer's or dementia.
Benefit Triggers and ADLs
You do not simply file a claim because you feel old or tired. A policy only activates when specific legal and medical thresholds are crossed. Benefit triggers in a Long-Term Care policy are the specific conditions that must occur for the policy to begin paying benefits.
To activate the policy, Long-Term Care policies typically require a physician to certify that the insured is chronically ill before triggering benefits.
Beyond the physician's certification, the mechanics of the policy rely on assessing the insured's physical autonomy. The inability to perform Activities of Daily Living is a primary benefit trigger for Long-Term Care policies. To standardize this across the industry, the standard Activities of Daily Living include bathing, dressing, eating, transferring, toileting, and continence.
As a producer, you must understand the exact definitions of these ADLs, as they represent the fundamental units of human independence:
- Bathing refers to the ability of an individual to wash oneself in a tub, shower, or by sponge bath.
- Dressing refers to the ability of an individual to put on and take off all necessary items of clothing.
- Eating refers to the ability of an individual to feed oneself. (Note: This is about the physical act of eating, not cooking or preparing the food).
- Transferring refers to the ability of an individual to move into or out of a bed, chair, or wheelchair.
- Toileting refers to the ability of an individual to get to and from the toilet and perform associated personal hygiene.
- Continence refers to the ability of an individual to maintain control of bowel and bladder function.
A Long-Term Care policy typically requires the inability to perform at least two Activities of Daily Living to trigger benefits.
However, a person with severe dementia might be physically perfectly capable of walking, eating, and dressing themselves, but they would wander into traffic if left alone. Because their physical ADLs are intact, they require a different pathway to coverage. Thus, severe cognitive impairment serves as a distinct, standalone benefit trigger for Long-Term Care policies.
Levels of Care
Once a policy is triggered, it will pay for various levels of intervention based on the insured's needs. The state exam expects you to distinguish between these clearly:
| Level of Care | Definition |
|---|---|
| Skilled Nursing Care | Provides daily medical care performed by registered nurses under the supervision of a physician. (e.g., changing sterile wound dressings, IV administration). |
| Intermediate Care | Provides occasional medical care performed by registered nurses under the supervision of a physician. (e.g., physical therapy three times a week). |
| Custodial Care | Provides assistance with Activities of Daily Living by non-medical personnel. (This is the most common LTC claim—helping a client bathe and dress). |
| Adult Day Care | Provides custodial care on less than a 24-hour basis outside of the insured individual's home. (Provides daytime supervision and social interaction). |
| Respite Care | Provides temporary relief for a primary family caregiver by paying for a substitute caregiver. (Allows a dedicated family member to take a weekend off to rest). |
Policy Mechanics and Provisions
Much like Medigap, LTC policies are heavily regulated to protect consumers. All Long-Term Care policies must provide a minimum 30-day free look period. Furthermore, individual Long-Term Care policies must be issued as guaranteed renewable, meaning coverage cannot be canceled as the client ages and their health declines, provided they pay the premium.
Financially, LTC policies do not usually pay from day one. Long-Term Care policies include an elimination period before benefits begin. Think of this as a deductible measured in time rather than dollars. The elimination period is a waiting period during which the insured must pay out-of-pocket for long-term care services. Common elimination periods are 30, 90, or 180 days. A longer elimination period lowers the monthly premium, but increases the out-of-pocket burden on the family when care first becomes necessary.
If LTC is about the slow, chronic decline of the body, AD&D is about the sudden, violent geometry of accidents.
Accidental Death and Dismemberment policies pay a lump sum benefit for accidental death or the loss of specific body parts. These are highly specific, narrow policies. Accidental Death and Dismemberment policies do not pay benefits for death or disability caused by illness or disease. If a client dies of a massive heart attack while driving and crashes their car, the primary cause of death is illness, and the AD&D policy will generally not pay.

Principal vs. Capital Sum
The payouts in an AD&D policy are categorized into two distinct sums:
- The Principal Sum: The principal sum in an Accidental Death and Dismemberment policy is the maximum payout amount triggered by accidental death. If a client buys a $100,000 AD&D policy, the principal sum is $100,000.
- The Capital Sum: The capital sum in an Accidental Death and Dismemberment policy is the payout amount triggered by accidental dismemberment.
The relationship between these two numbers is mathematical: The capital sum is expressed as a percentage of the principal sum. For example, the loss of one arm might pay 50% of the principal sum (a $50,000 capital sum payout).
Defining Time and Severance
Insurance contracts abhor ambiguity. If a client is in a car accident, slips into a coma, and dies three years later, did the accident cause the death, or did intervening medical issues cause it? To sever this ambiguity, Accidental Death and Dismemberment policies usually require the death or dismemberment to occur within 90 days of the accident.
Furthermore, what defines "dismemberment"? A broken arm or a paralyzed leg does not traditionally qualify. By standard definition, accidental dismemberment typically requires the physical severance of a limb (often defined as severance at or above the wrist or ankle joint).
There is one notable exception to the physical severance rule: vision. Accidental Death and Dismemberment policies define the total loss of sight as a dismemberment qualifying for the capital sum.
Finally, we address the transient gaps in the healthcare system. Imagine a client who has just graduated college and is waiting for their corporate health benefits to kick in three months from now, or a client who was laid off and cannot afford COBRA premiums.
Short-term medical policies provide temporary health insurance coverage for individuals experiencing a gap in long-term coverage. Think of these policies as the "spare tire" in the trunk of a car. A spare tire is not meant for a cross-country road trip; it is meant to keep the car rolling for 50 miles until you can get a real tire.
Because they are temporary stopgaps, short-term medical policies typically offer coverage durations ranging from one month to less than one year. (State regulations vary on exact duration limits, but fundamentally, they are designed to be temporary).
The Limitations of the "Spare Tire"
Because short-term policies are priced highly affordably, they lack the robust protections of standard Major Medical insurance. You must clearly explain to clients what these policies do not do:
- No Renewal Guarantees: Short-term medical policies are not guaranteed renewable. When the term ends, the policy expires. If the client became sick during the term, the insurer is not obligated to offer them a new policy.
- No Pre-existing Conditions: Short-term medical policies exclude coverage for pre-existing conditions. If a client has asthma, their inhalers or hospitalizations related to asthma will not be covered.
- Exempt from Federal Mandates: Because they are temporary, short-term medical policies are not required to cover the essential health benefits mandated by the Affordable Care Act.
- Specific Exclusions: To keep premiums low, carriers strip out expensive, high-utilization benefits. Consequently, short-term medical policies generally exclude maternity care coverage and short-term medical policies generally exclude mental health services coverage.
Understanding these limitations is vital. A short-term policy will protect a client from bankruptcy if they get hit by a bus while between jobs, but it will not pay for routine therapy, a normal pregnancy, or a pre-existing heart condition.

By mastering the mechanics of Medigap, Long-Term Care, AD&D, and Short-Term Medical policies, you do more than pass an exam. You gain the ability to accurately diagnose a client's specific vulnerability and deploy the exact financial instrument required to secure their future.