Fundamentals of Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
The modern hospital ward is a high-stakes ecosystem of competing variables, where entropy constantly threatens to overtake physiological stability. A nurse managing four acute patients is not merely performing a sequence of tasks; they are operating as a real-time triage engine, calculating probabilities, assessing risks, and applying interventions based on immutable laws of clinical priority. In this environment, recognizing that an unmaintained airway will cause irreversible cerebral ischemia long before a missed dose of antibiotics affects a systemic infection is not just intuition—it is the applied science of human survival. Mastering the fundamentals of nursing practice for the Saudi Nursing Licensure Examination (SNLE) requires a deep structural understanding of prioritization, the rigorous algorithm of the nursing process, and the non-negotiable ethical and legal boundaries that govern professional accountability in the Kingdom of Saudi Arabia.
When multiple systems demand your attention simultaneously, you need an absolute, objective framework to determine what happens first. In nursing, we rely on two primary models: Maslow's Hierarchy of Needs and the ABC framework. Think of these as the laws of thermodynamics for patient care—you cannot cheat them.
Maslow's Hierarchy Applied to Clinical Care
Maslow's hierarchy of needs dictates that basic physiological needs must be met before addressing higher-level psychological needs. You cannot effectively teach a patient about their new diabetes diet if they are gasping for air.
- Physiological Needs: This is the bedrock of survival. Physiological needs in Maslow's hierarchy include oxygen, water, food, sleep, elimination, and shelter.
- Safety and Security: Once the physiological baseline is established, we move to safety. Safety and security needs in Maslow's hierarchy involve protecting the patient from physical harm and psychological distress. This includes fall precautions, infection control, and establishing a trusting environment.
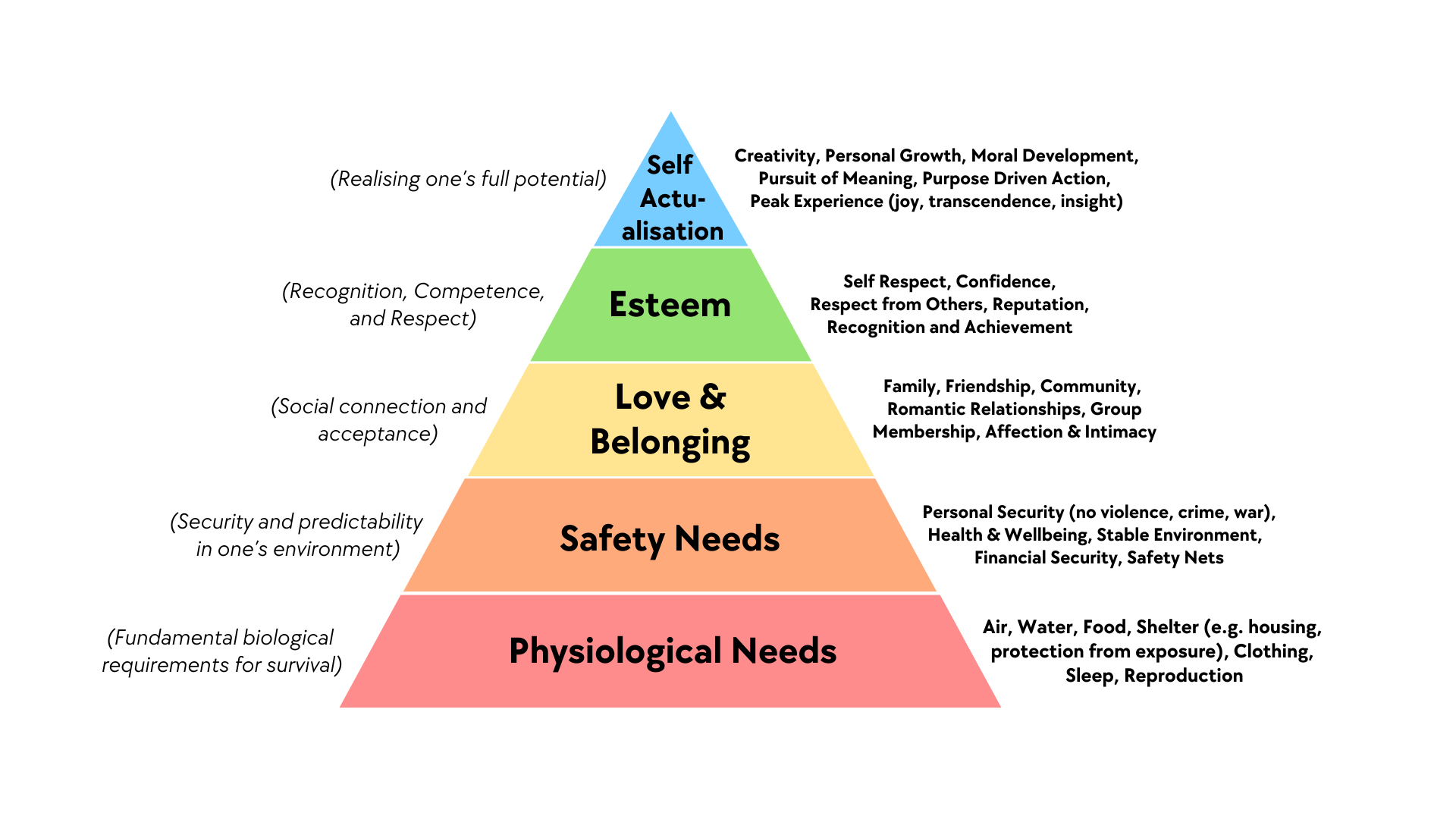
When managing a patient assignment, the rule of thumb is strict: Urgent physiological needs like acute pain and fluid imbalances take priority over a patient's need for love and belonging. A patient anxious about their family visiting (love and belonging) must wait if your other patient is experiencing acute hypovolemia (fluid imbalance).
The ABC Framework: The Immediate Flow of Life
If Maslow tells us to focus on the physiological, the ABC framework tells us which physiological process matters most. The human body relies on a continuous supply chain of oxygen.
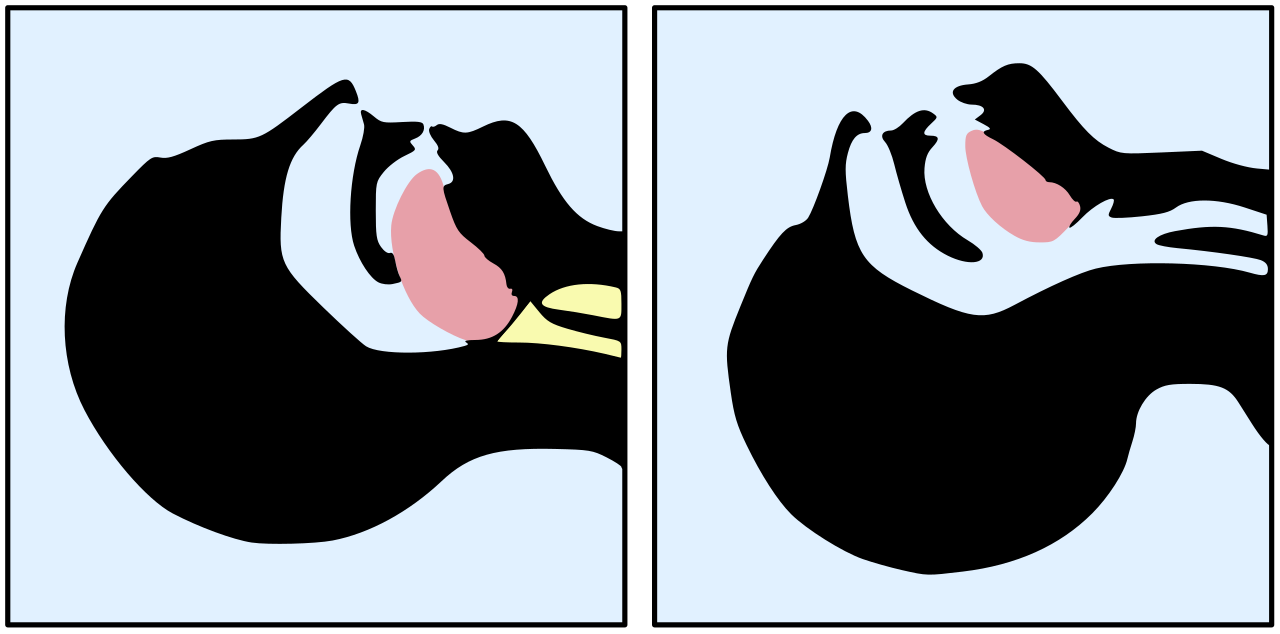
- Airway: The pipe must be open. The ABC priority framework requires nurses to secure a patient's airway before assessing breathing. If the trachea is obstructed, evaluating the respiratory rate is entirely pointless.
- Breathing: The bellows must pump. Once the airway is clear, the ABC priority framework requires nurses to stabilize a patient's breathing before addressing systemic circulation issues.
- Circulation: The pump must distribute the oxygenated blood.
The Three Tiers of Clinical Priority
To apply these frameworks on the ward, we categorize problems into three distinct levels:
First-level priority problems include immediate threats to survival such as airway obstruction or cardiac arrest. These demand instantaneous intervention.
Second-level priority problems include acute clinical changes like abnormal laboratory values or untreated severe pain. These will deteriorate into first-level problems if ignored.
Third-level priority problems encompass long-term health management issues like patient education and discharge planning. These are critical for holistic care but are addressed only when the patient is physiologically stable.
Every scientific discipline has a method for solving problems. In nursing, this algorithmic approach is known as the nursing process.
The nursing process consists of five distinct phases including assessment, diagnosis, planning, implementation, and evaluation. (Often remembered by the acronym ADPIE).
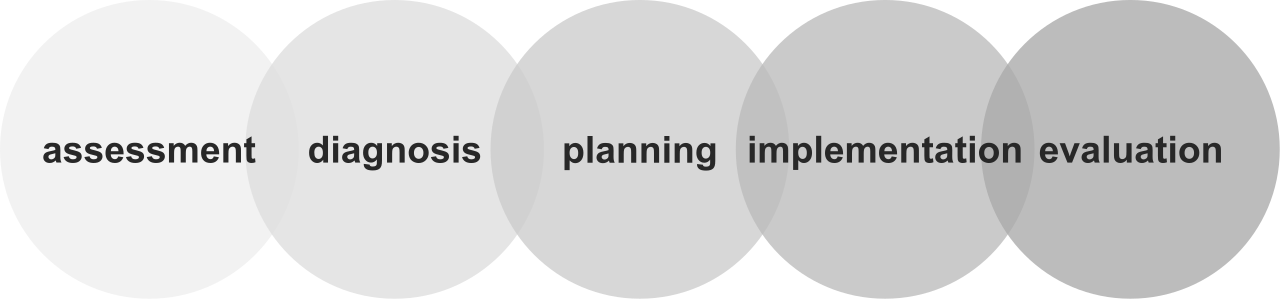
The most unbreakable rule of this process relates to its sequencing: Assessment must always be the first step completed in the nursing process before planning any clinical interventions.
Imagine a mechanic trying to replace an engine block without first opening the hood to see if the battery is simply dead. Acting without assessing is clinically dangerous. Whether a patient's blood pressure drops, or they complain of sudden nausea, your first action is always to gather data. You must define the parameters of the problem before you attempt to solve it.
Clinical skill without ethical grounding is dangerous. As a registered professional, you operate under a strict code of conduct. Accountability in nursing requires the individual nurse to take full legal and ethical responsibility for all professional actions. You cannot blame the system, the physician, or the shift before you.
Core Ethical Principles
To be a professional is to uphold these six pillars:
- Autonomy is the ethical principle that recognizes a patient's fundamental right to make independent healthcare decisions decisions. We advise, but the patient steers their own ship.
- Beneficence is the ethical principle of acting in ways that actively promote the well-being and health of others. It is the active pursuit of good.
- Non-maleficence is the core ethical principle that obligates healthcare providers to do no harm to their patients. This means double-checking medications and maintaining sterile fields.
- Justice is the ethical principle demanding fairness and equity in the distribution of scarce healthcare resources. Triage is based on clinical need, never on social status.
- Veracity is the ethical principle that requires healthcare providers to tell the truth and avoid deceiving patients. Trust is built on transparency.
- Fidelity is the ethical principle of keeping promises and maintaining strict trust in the nurse-patient relationship. If you tell a patient you will return in ten minutes with pain medication, you return in ten minutes.
The Legal Boundaries: Torts and Violations
When ethical principles are breached, they often cross into legal violations.
- Negligence vs. Malpractice: Negligence is a failure to exercise the standard of care that a reasonably prudent nurse would provide in a similar situation. If you fail to put up the bed rails for a confused patient, that is negligence. However, malpractice is defined legally as professional negligence that directly results in patient injury or harm. If that same patient falls out of bed and fractures their hip, the negligence has evolved into malpractice.
- Assault vs. Battery: These two are often confused. Assault is an intentional threat to cause bodily harm that creates a fear of imminent danger in the patient. (e.g., "If you don't stay still, I will force this tube down your throat.") Conversely, battery is defined as the intentional and unauthorized physical contact with a patient. Therefore, administering an intravenous medication against a legally competent patient's direct refusal constitutes battery, regardless of how much they clinically need the medication.
- False Imprisonment: This tort is related to a violation of autonomy and freedom of movement. False imprisonment involves unlawfully restraining a patient against the patient's explicitly stated will, such as tying a competent patient to the bed to prevent them from leaving against medical advice.
The Mechanics of Informed Consent
Consent is a vital intersection of autonomy, law, and clinical practice. Informed consent requires that the patient is fully educated about the specific risks and benefits of a procedure before agreeing.
It is crucial to understand the distinct roles here. Obtaining the actual informed consent for a surgical or invasive medical procedure is the legal responsibility of the physician who is performing it. The nurse cannot explain the risks of a complex cardiac catheterization. Instead, a registered nurse acts solely as a legal witness to the patient's signature on a medical informed consent form, verifying that the patient signed voluntarily and appears competent to do so.
Practicing nursing in Saudi Arabia requires an exquisite sensitivity to the intersection of modern medicine, Islamic bioethics, and local cultural norms. Cultural competence requires providing holistic care that carefully aligns with the patient's religious and cultural beliefs.
Preservation of Life and DNAR Orders
Islamic bioethics prioritize the preservation of human life above many other competing clinical considerations. Because of this immense value placed on life, the threshold for withdrawing or withholding life-sustaining treatment is exceptionally high.
Unlike in some Western jurisdictions where a single attending physician might write an order, a valid Do Not Attempt Resuscitation order in Saudi Arabia requires the documented agreement and signatures of three consultant physicians. This rigorous legal standard ensures that the decision is scientifically sound and ethically justified.
Modesty, Family, and Patient Privacy
The sociocultural fabric of the Kingdom heavily influences daily ward operations.
- Modesty: Observing physical modesty and maintaining gender concordance between the nurse and patient is highly valued in Saudi Arabian healthcare settings. Whenever clinically feasible, assigning female nurses to female patients and male nurses to male patients builds immense trust and comfort.
- Family Dynamics: Western bioethics heavily emphasizes pure individual autonomy. However, extended family members often play a central collaborative role in complex healthcare decision-making for patients in Middle Eastern cultures.
- Confidentiality: Despite the familial involvement, legal privacy remains paramount. The Saudi Ministry of Health mandates strict adherence to patient privacy and confidentiality regarding all electronic and paper medical records. You cannot disclose information to family members without the patient's explicit consent.
Navigating Religious Practices on the Ward
Accommodating religious obligations is not a courtesy; it is a core component of therapeutic care.
-
Dietary Restrictions: Hospital nutrition must adhere to Islamic law. Halal dietary guidelines strictly prohibit the consumption of pork products, blood, and alcohol.
-
Daily Prayer: Prayer (Salah) is performed five times a day. Practicing Muslim patients often prefer their hospital bed or chair to face the Qibla during daily prayer times. Assisting a patient to position themselves or providing a clean space for prayer demonstrates high-level cultural competence.
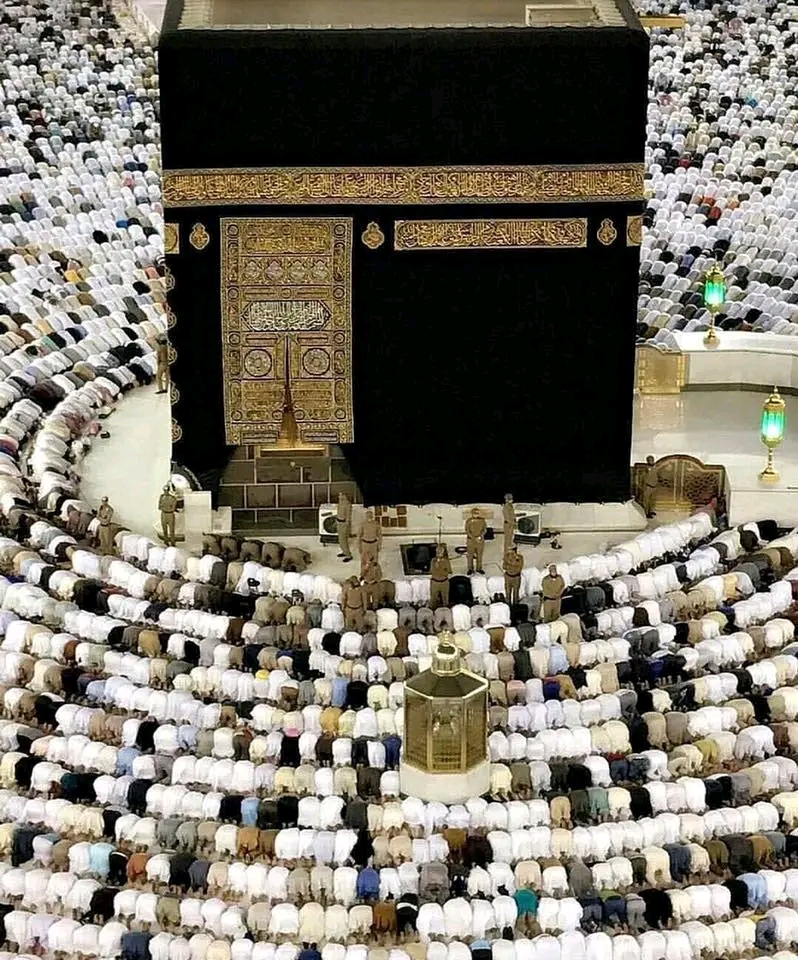
During the five daily prayers (Salah), Muslim patients orient themselves toward the Kaaba in Mecca, known as the Qibla. Accommodating this physical positioning is a core aspect of culturally competent nursing care in Saudi Arabia. Source: Kaaba 2 by mabruuk, CC BY-SA 4.0. -
Ramadan Modifications: The holy month of Ramadan presents a unique clinical challenge. Adult Muslim patients may request to fast from food, water, and oral medications from dawn until sunset during the month of Ramadan. Instead of merely documenting non-compliance if a patient refuses a noon medication, nurses must proactively coordinate with the prescribing physician to safely adjust medication schedules for a patient fasting during Ramadan (e.g., shifting once-daily doses to after sunset).
No nurse operates alone. We amplify our impact through teamwork, which requires delegation. Delegation is the specific process of transferring the performance of a designated nursing task to a competent individual (like a licensed practical nurse or unlicensed assistive personnel).
However, you transfer the task, not the responsibility. The registered nurse retains ultimate legal accountability for the patient outcome of any delegated nursing task.
Because you retain accountability, there are strict limits to what you can hand off: A registered nurse cannot legally delegate the core nursing tasks of clinical assessment, nursing diagnosis, or care planning. You can delegate taking vital signs, but you cannot delegate the interpretation of those vital signs.
The Five Rights of Delegation
To delegate safely, a nurse must act like an air traffic controller, ensuring every variable aligns perfectly before clearing a task. We use a checklist:
The Five Rights of Delegation include:
- Right Task: Is this task legally delegable and appropriate for this specific patient?
- Right Circumstance: Is the patient stable? (Do not delegate vital signs on a crashing patient).
- Right Person: Does the delegatee possess the verified competency to do this?
- Right Direction: Did you provide clear, specific instructions and parameters for reporting back?
- Right Supervision: Are you actively monitoring the outcome?
If you delegate feeding a patient to a nursing assistant, and you notice the assistant feeding the patient while they are lying flat, you cannot simply document it later. A registered nurse must intervene immediately if a delegated task is being performed unsafely by unlicensed assistive personnel. You own the environment, you own the patient's safety, and you own the outcome.