Neonatal Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Imagine a spacecraft re-entering Earth’s atmosphere. The external environmental support system is suddenly severed, and the vessel's internal engines must instantly ignite to sustain life. When a human infant is born, the placenta—their biological life-support system for nine months—is cut. In mere seconds, the neonate must inflate collapsed lungs, reroute systemic cardiac blood flow, ignite independent metabolism, and defend against a sudden, drastic drop in ambient temperature. As a nurse preparing for the Saudi Nursing Licensure Examination (SNLE), mastering neonatal care requires looking beyond isolated pediatric parameters. Your role on the postpartum ward or the Neonatal Intensive Care Unit (NICU) is to monitor and protect this extraordinary physiological transition.

To understand if our neonate has successfully made the transition to extrauterine life, we must perform an immediate engine check.
The Apgar scoring system evaluates heart rate, respiratory effort, muscle tone, reflex irritability, and skin color. These five parameters provide a rapid, standardized snapshot of the infant's cardiopulmonary and neurological adaptation. The Apgar score is assessed at 1 minute and 5 minutes after birth.
If you calculate an Apgar score of 7 to 10, this indicates a neonate in good condition requiring only routine care. Lower scores demand immediate, escalating resuscitation.
Once stabilized, we monitor the baseline telemetry. Neonatal vital signs operate at a much higher metabolic velocity than adult vitals:
- Normal neonatal heart rate ranges from 110 to 160 beats per minute while the infant is awake.
- Normal neonatal respiratory rate ranges from 30 to 60 breaths per minute.
- Normal neonatal axillary temperature ranges from 36.5 to 37.5 degrees Celsius.
Because the respiratory control center in the brainstem is still maturing, irregular breathing patterns can occur. However, you must differentiate normal irregularity from pathological pauses. Neonatal apnea is defined as a cessation of breathing lasting longer than 20 seconds. Anything shorter is generally considered a normal periodic breathing pattern, but a pause exceeding 20 seconds is a physiological red flag demanding intervention.
Once the neonate is stable, you perform a head-to-toe structural and neurological assessment. Think of this as inspecting the hardware and the wiring.
The Cranial Pressure Gauges
The neonatal skull is not a solid vault; it is constructed of floating tectonic plates connected by fibrous sutures, allowing the head to compress during birth and the brain to grow afterward. The spaces where these sutures intersect are the fontanels, which serve as direct clinical pressure gauges for the infant's fluid volume and neurological status.
- The anterior fontanel in a healthy neonate is diamond-shaped and is the larger of the two. The anterior fontanel normally closes between 12 and 18 months of age.
- The posterior fontanel in a healthy neonate is triangle-shaped and much smaller. The posterior fontanel normally closes between 2 and 3 months of age.
When assessing a resting infant, these fontanels should be flat and soft.
Clinical Correlate: A bulging fontanel in a resting neonate indicates increased intracranial pressure (e.g., meningitis, hydrocephalus), whereas a depressed fontanel in a neonate indicates dehydration, signaling that the systemic fluid volume has collapsed.

The Umbilical Lifeline
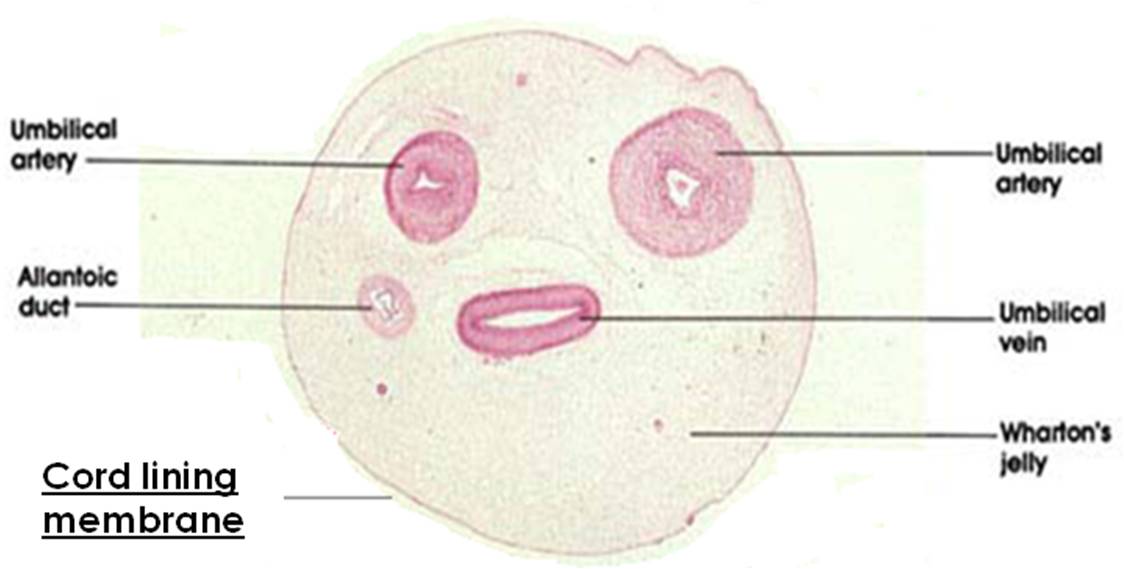
The umbilical cord was the primary conduit for oxygen and nutrients. A normal umbilical cord contains two arteries and one vein (easily remembered by the acronym AVA). Inspecting the cord for these three vessels is crucial, as the absence of one artery is frequently correlated with congenital renal anomalies.
Neurological Wiring: Neonatal Reflexes
Reflexes tell us if the central nervous system is accurately communicating with the peripheral musculoskeletal system.
The Moro reflex is elicited by a sudden loud noise or a sudden dropping of the neonate's head slightly backward. A normal Moro reflex involves symmetric extension and abduction of the arms followed by flexion (as if the baby is trying to embrace something). We are looking for symmetry. If the left arm extends but the right arm remains flaccid, the wiring or scaffolding is broken. Therefore, an asymmetric Moro reflex suggests a fractured clavicle or brachial plexus injury, highly relevant in difficult deliveries involving shoulder dystocia.
The Babinski reflex is elicited by stroking the lateral sole of the neonate's foot from the heel upward and across the ball of the foot. In an adult, a normal response is the downward curling of the toes. However, due to incomplete myelination of the neonatal corticospinal tracts, a normal Babinski reflex in a neonate involves fanning and extension of the toes.

Neonates are born with specific physiological gaps. We bridge these gaps before they leave the delivery room or the hospital.
- Vitamin K: The neonatal gut is sterile at birth. It lacks the normal bacterial flora required to synthesize Vitamin K, which is essential for the hepatic cascade of clotting factors. Therefore, intramuscular phytonadione is administered to neonates to prevent hemorrhagic disease of the newborn.

- Eye Care: During a vaginal delivery, the infant's eyes are exposed to the maternal flora of the birth canal. Prophylactic erythromycin ophthalmic ointment is administered to neonates to prevent gonococcal and chlamydial conjunctivitis, which can rapidly cause irreversible blindness.
- Immunization: To protect the infant's immature immune system from long-term liver pathology, the first dose of the Hepatitis B vaccine is routinely administered to neonates before hospital discharge.
- Metabolic Screening: We must verify that the infant does not have hidden enzymatic defects (like Phenylketonuria or congenital hypothyroidism). Newborn metabolic screening via heel stick is optimally performed after 24 hours of age, ensuring the baby has ingested enough breast milk or formula for metabolic errors to become detectable. Warming the neonate's heel before a capillary blood draw increases blood flow to the area and improves sample collection, preventing the need for multiple painful sticks.

One of the most profound concepts on the SNLE is the interconnected triad of temperature, glucose, and oxygen. If one fails, they all cascade into failure.
Adults shiver when they are cold to generate heat. Neonates cannot shiver. Instead, they rely on a unique physiological mechanism called non-shivering thermogenesis. To do this, they burn a highly vascularized adipose tissue called brown fat.
- Premature neonates lack adequate brown fat compared to full-term neonates.
- Because of this, a lack of brown fat impairs a premature neonate's ability to maintain thermoregulation through non-shivering thermogenesis.
If an infant is exposed to a cold environment, they experience cold stress. Cold stress in a neonate significantly increases oxygen consumption as the body desperately tries to fuel brown fat metabolism. Simultaneously, cold stress in a neonate rapidly depletes glucose stores. A cold baby quickly becomes a hypoxic and hypoglycemic baby.
Managing Hypoglycemia
Neonatal hypoglycemia is generally defined as a blood glucose level less than 40 mg/dL. Neonates born to diabetic mothers are at high risk for developing hypoglycemia shortly after birth. Why? In in utero, the mother's high blood sugar crossed the placenta, causing the fetal pancreas to pump out massive amounts of insulin. When the umbilical cord is cut, the glucose supply abruptly stops, but the neonate's hyperactive pancreas is still releasing high levels of insulin, which violently crashes their blood sugar.
Assessment Alert: Jitteriness, lethargy, and poor feeding are primary clinical signs of neonatal hypoglycemia. If you see a jittery newborn on the ward, immediately check a capillary blood glucose.
Preventing Cold Stress
To combat cold stress, especially in premature infants, nurses utilize both incubators and human biology. Kangaroo care involves placing the diaper-clad neonate skin-to-skin on the parent's bare chest. This simple, profound intervention acts as a highly efficient bio-incubator: Kangaroo care promotes thermoregulation and stabilizes heart rate in premature infants.

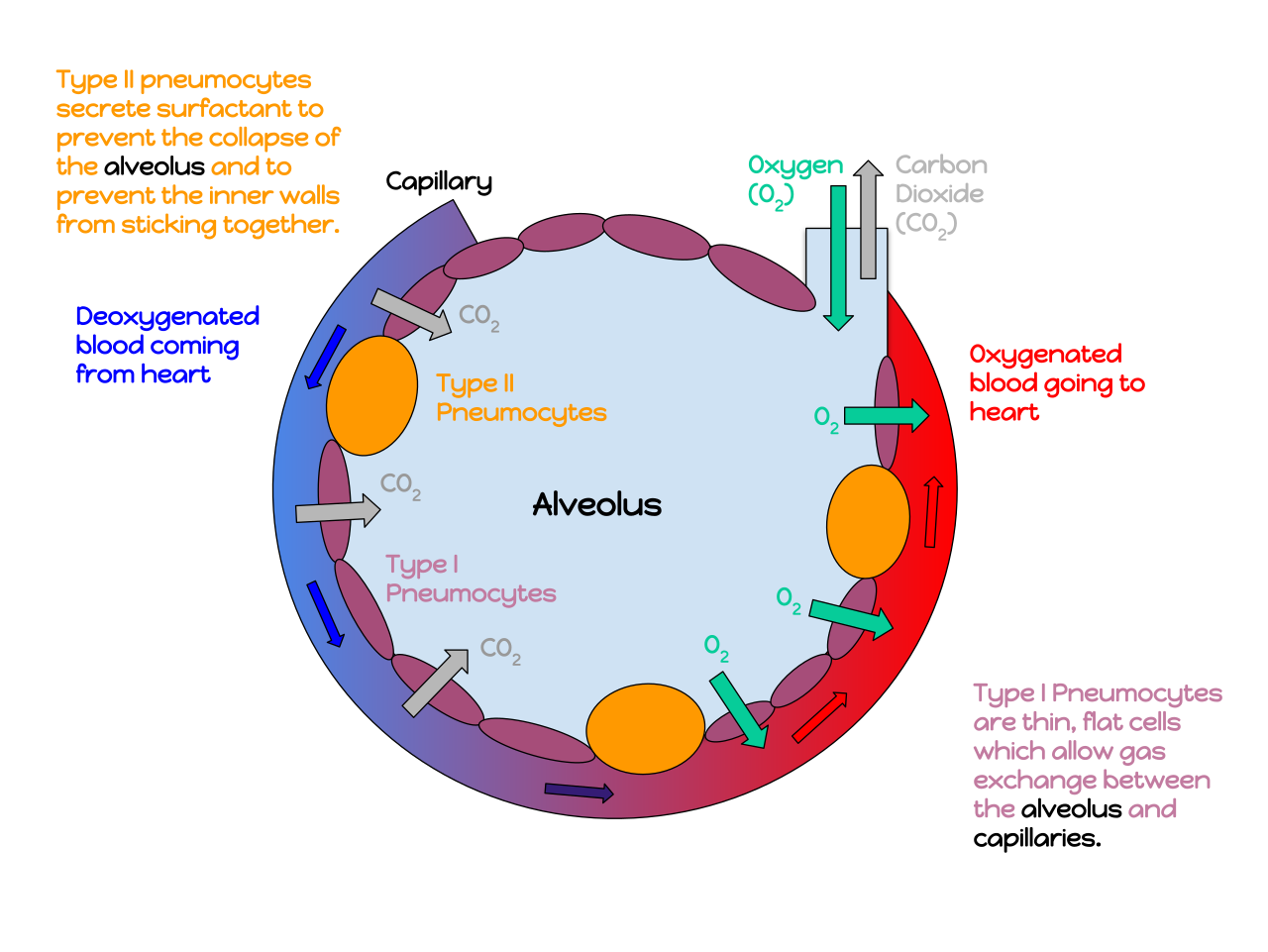
Respiratory Distress Syndrome (RDS)
If oxygen pathways fail natively, the infant enters respiratory distress. Respiratory Distress Syndrome primarily occurs in premature infants due to a lack of pulmonary surfactant, the soapy substance that keeps the alveoli from collapsing during exhalation. Expiratory grunting, nasal flaring, and intercostal retractions are classic signs of neonatal respiratory distress. Grunting is the baby's attempt to create their own positive end-expiratory pressure (PEEP) against a closed glottis to keep the alveoli open.
When an infant's systems are compromised, the presentation is uniquely neonatal.
Neonatal Sepsis
Adults mount a massive febrile response to infection. A neonate's immune system is far too immature to mount a reliable fever. Instead, neonatal sepsis often presents with temperature instability rather than a true fever. Often, the first sign of profound systemic infection is hypothermia.
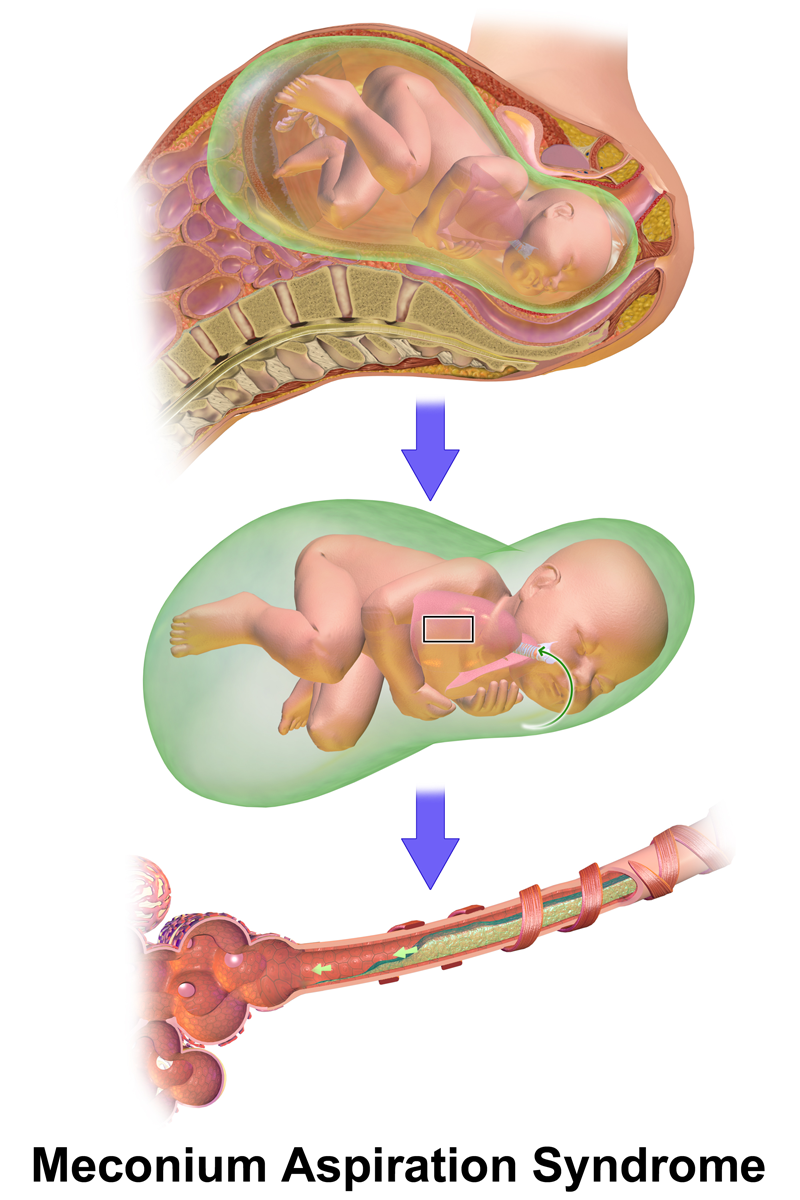
Meconium Aspiration Syndrome (MAS)
If a fetus is stressed in utero (often due to hypoxia), its anal sphincter may relax, passing the first stool (meconium) into the amniotic fluid. Meconium aspiration syndrome occurs when a fetus inhales meconium-stained amniotic fluid before or during birth. This thick, tarry substance physically blocks airways and causes severe chemical pneumonitis.
Hyperbilirubinemia (Jaundice)
Neonatal red blood cells have a short lifespan and break down quickly, releasing large amounts of bilirubin. The immature neonatal liver often struggles to conjugate this bilirubin for excretion, leading to jaundice. The timing of the yellowing skin dictates our clinical concern:
- Pathologic jaundice appears within the first 24 hours of life. This is an emergency, often caused by blood group incompatibilities (Rh or ABO) causing massive hemolysis.
- Physiologic jaundice typically appears after the first 24 hours of life. This is a normal, transient delay in liver clearance.
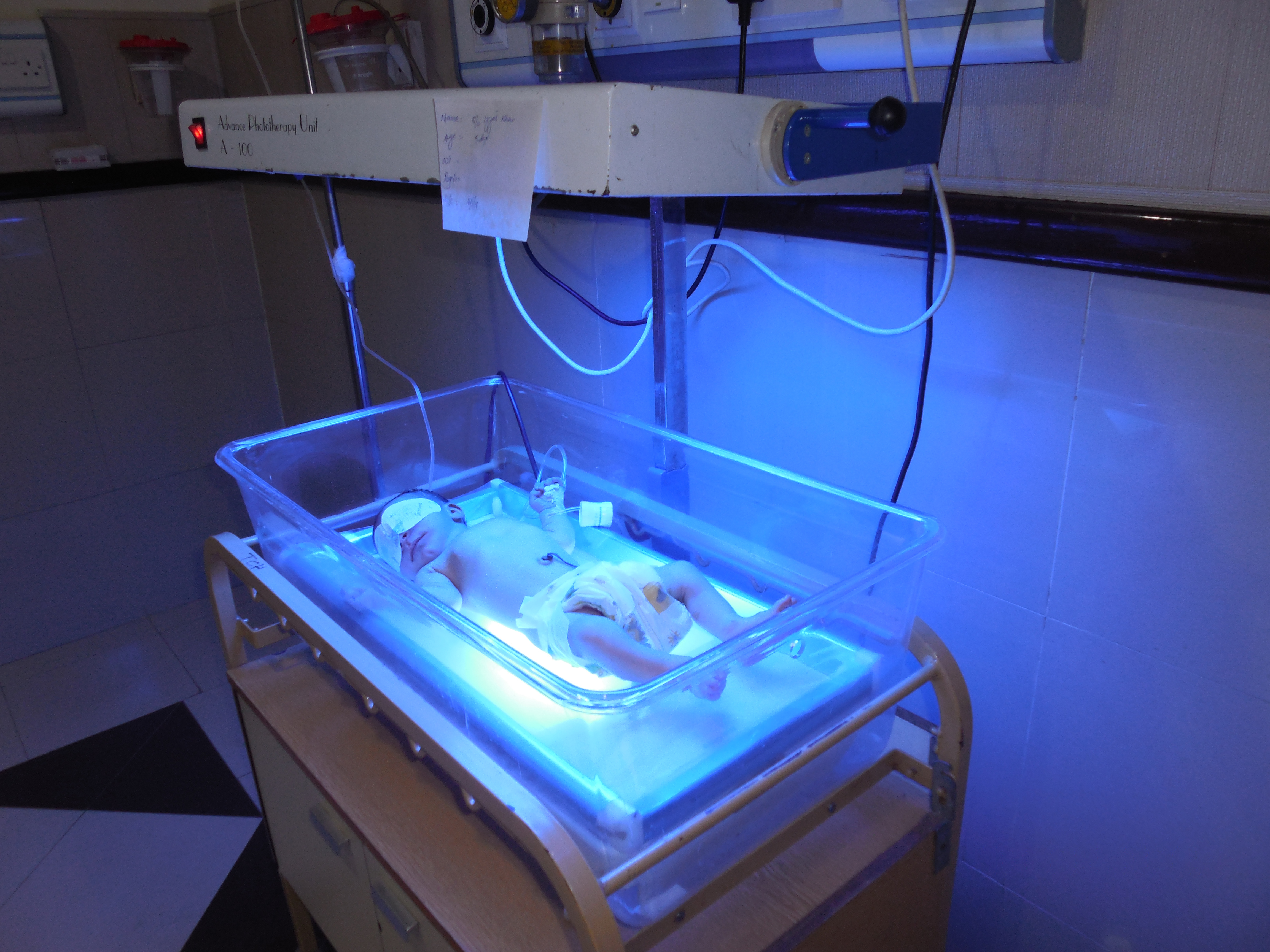
When bilirubin levels rise dangerously, we intervene with light. Phototherapy treats hyperbilirubinemia by converting unconjugated bilirubin into a water-soluble form for excretion through the urine and feces. While under the lights, patient safety is paramount:
- The nurse must place opaque eye patches on a neonate during phototherapy to prevent retinal damage.
- Because the lights increase insensible water loss through the skin, the nurse must closely monitor a neonate undergoing phototherapy for signs of dehydration.
The final pillar of neonatal nursing involves establishing safe home routines and empowering the parents.
Facilitating the Maternal-Infant Bond
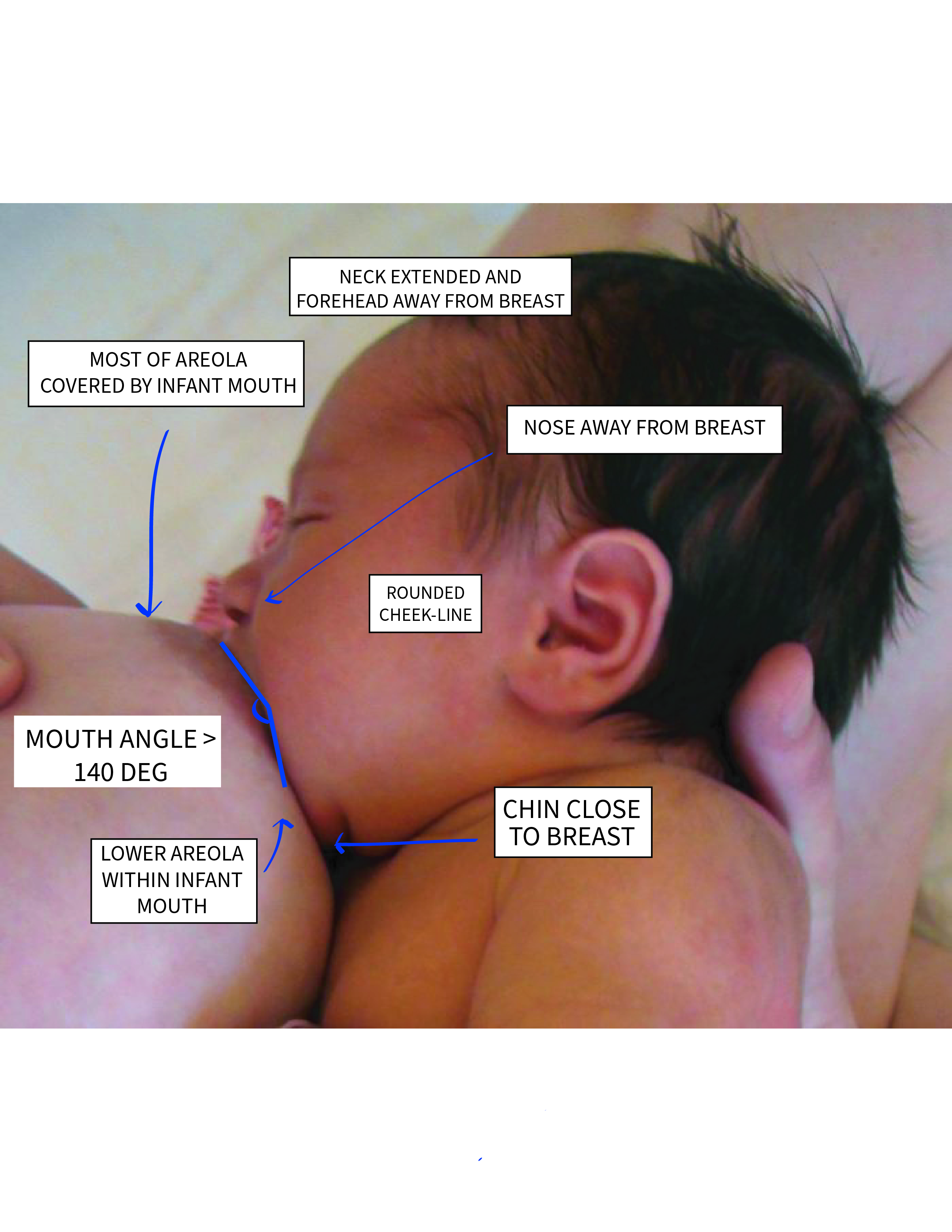
Early nutrition is inseparable from maternal bonding. The World Health Organization recommends initiating breastfeeding within the first hour of life.
To succeed at breastfeeding, mothers must learn to speak their baby's physical language. Rooting, smacking lips, and bringing hands to the mouth are early hunger cues in neonates. A common pitfall is waiting for the baby to vocalize distress. Crying is a late sign of hunger in neonates, and a frantically crying baby will struggle to latch effectively.
To help the mother learn these early cues, hospitals utilize a specific environmental design. Rooming-in allows the mother and neonate to remain together in the same room throughout the hospital stay. Being in close proximity is not just for bonding; rooming-in facilitates maternal recognition of early infant feeding cues.
Safe Sleep
As nurses, protecting the infant extends beyond the hospital walls. To prevent Sudden Infant Death Syndrome (SIDS), neonates must be placed entirely on their backs to sleep. Furthermore, the neonatal sleep environment must be free of soft bedding, stuffed animals, and bumper pads to reduce suffocation risk. The crib should contain only a firm mattress and a tightly fitted sheet.

Healing: Circumcision and the Umbilical Cord
Finally, you will frequently instruct parents on proper wound care.
Umbilical Cord Care: The umbilical cord stump must be kept dry and exposed to room air to promote healing. Parents must not use harsh antiseptics. To protect the stump from maceration and infection, the neonate's diaper should be folded below the umbilical cord stump to prevent contamination with urine. Over time, the stump will dry, turn black, and naturally detach. The umbilical cord stump typically detaches and falls off within 10 to 14 days after birth.

Circumcision Care (Gomco Clamp): If a male infant undergoes a Gomco clamp circumcision, the mucosal surface of the glans penis is exposed and vulnerable. Petroleum jelly is applied to the glans penis after a Gomco clamp circumcision to prevent the diaper from adhering to the site and tearing the newly forming tissue. Within 24 hours, you will notice a yellowish film forming over the glans. This frequently alarms parents, who mistake it for purulent drainage. However, yellow exudate on the glans penis after circumcision is a normal part of the healing process, representing granulation tissue. You must educate parents and enforce a strict protocol: The nurse must strictly avoid forcibly removing yellow exudate from a healing circumcision site, as doing so will cause hemorrhage and disrupt primary wound healing.