Physical Assessment
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
A skilled nurse stepping into a patient room on a bustling medical-surgical ward in Riyadh is fundamentally an investigative scientist. The physical assessment process begins the moment the nurse first encounters the patient. Before a single instrument is touched or a specific question is asked, the general survey captures a wealth of foundational clinical information. The general survey is the first component of the physical assessment, and it includes observations of the patient's physical appearance, body structure, mobility, and behavior. By merely watching a patient breathe, move to the edge of the bed, or respond to an initial greeting, you are gathering vital evidence.
These observations yield objective data, which consists of measurable physical findings observed by the healthcare provider. We contrast this with subjective data, which consists of the specific symptoms and feelings reported directly by the patient—their personal experience of the illness. To succeed on the SNLE and provide exceptional care in Saudi Arabia, you must master the mechanics of gathering this objective data while adapting your approach to respect the diverse populations and cultural expectations you will encounter daily.
In the Kingdom, clinical excellence is inseparable from cultural respect. Islamic cultural values require the nurse to maintain patient modesty by exposing only the specific body part being actively assessed. This is not merely a courtesy; it is a foundational pillar of patient trust and psychological safety. Furthermore, when a male healthcare provider assesses a female patient in the Saudi healthcare setting, the nurse must seek a same-gender chaperone. This ensures that the patient feels secure and that professional boundaries are irreproachably maintained.
Physical assessment relies on the nurse’s senses—sight, touch, hearing—enhanced by clinical tools. The standard sequence of physical assessment techniques is inspection, palpation, percussion, and auscultation. You look, you feel, you tap, and you listen.
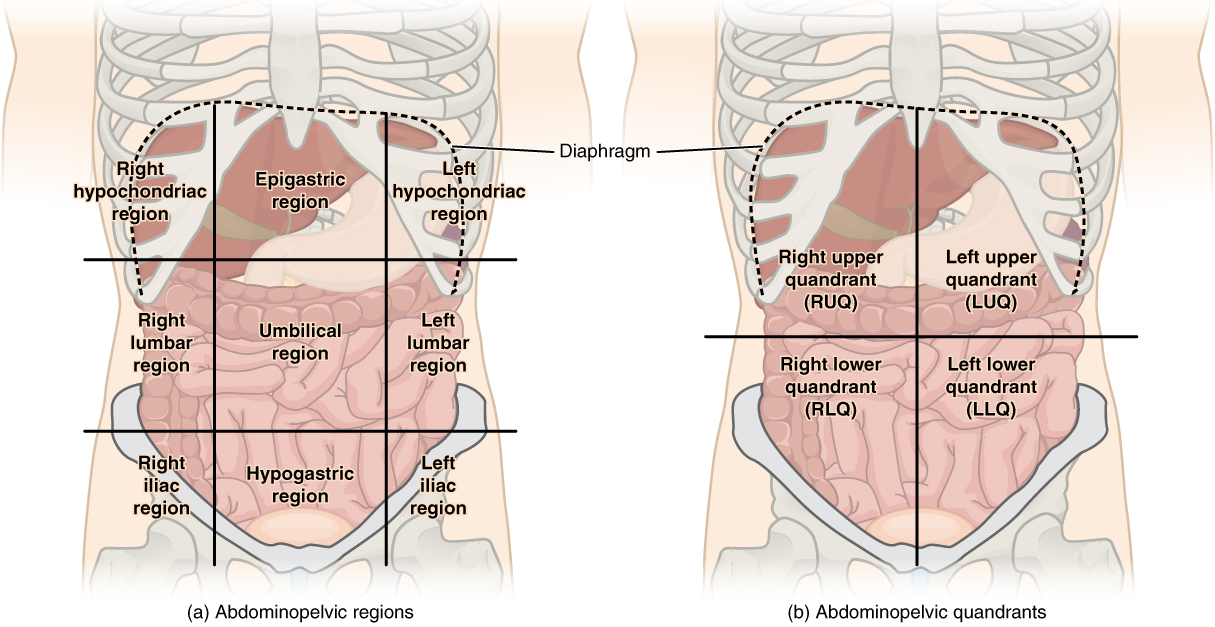
However, the laws of physics and physiology demand a critical exception for the gastrointestinal system. The physical assessment sequence for the abdomen is inspection, auscultation, percussion, and palpation. Why do we invert the order? Because auscultating the abdomen before palpation prevents the artificial stimulation of bowel sounds. If you press into the patient's abdomen first, you displace fluid and gas, creating mechanical noise that obscures the true baseline of intestinal motility.
The Mechanics of Touch: Palpation
When palpating, your hand is a highly calibrated sensor array, and different regions of your hand serve different analytical purposes:
- The fingertips are the most sensitive part of the hand for fine tactile discrimination during palpation (e.g., assessing the texture of a mass or feeling a pulse).
- The dorsal surface of the hand (the back of the hand), where the skin is thinner, is the most sensitive area for assessing the patient's skin temperature.
- The ulnar surface of the hand (the base of the fingers/palm) is the most sensitive area for detecting vibrations during palpation, such as the tactile fremitus of a speaking patient.
The Science of Sound: Percussion and Auscultation
Percussion involves tapping the patient's skin with short strokes to assess the density of underlying structures. Think of it as medical sonar. The sound that reflects back tells you what lies beneath the surface:
| Percussion Note | Acoustic Quality | Physiological Meaning |
|---|---|---|
| Tympany | Hollow sound | Commonly heard over a gas-filled stomach or air-filled intestine. |
| Resonance | Low-pitched sound | Heard over healthy adult lung tissue. |
| Dullness | Muffled sound | Normally heard over dense organs like the liver. |
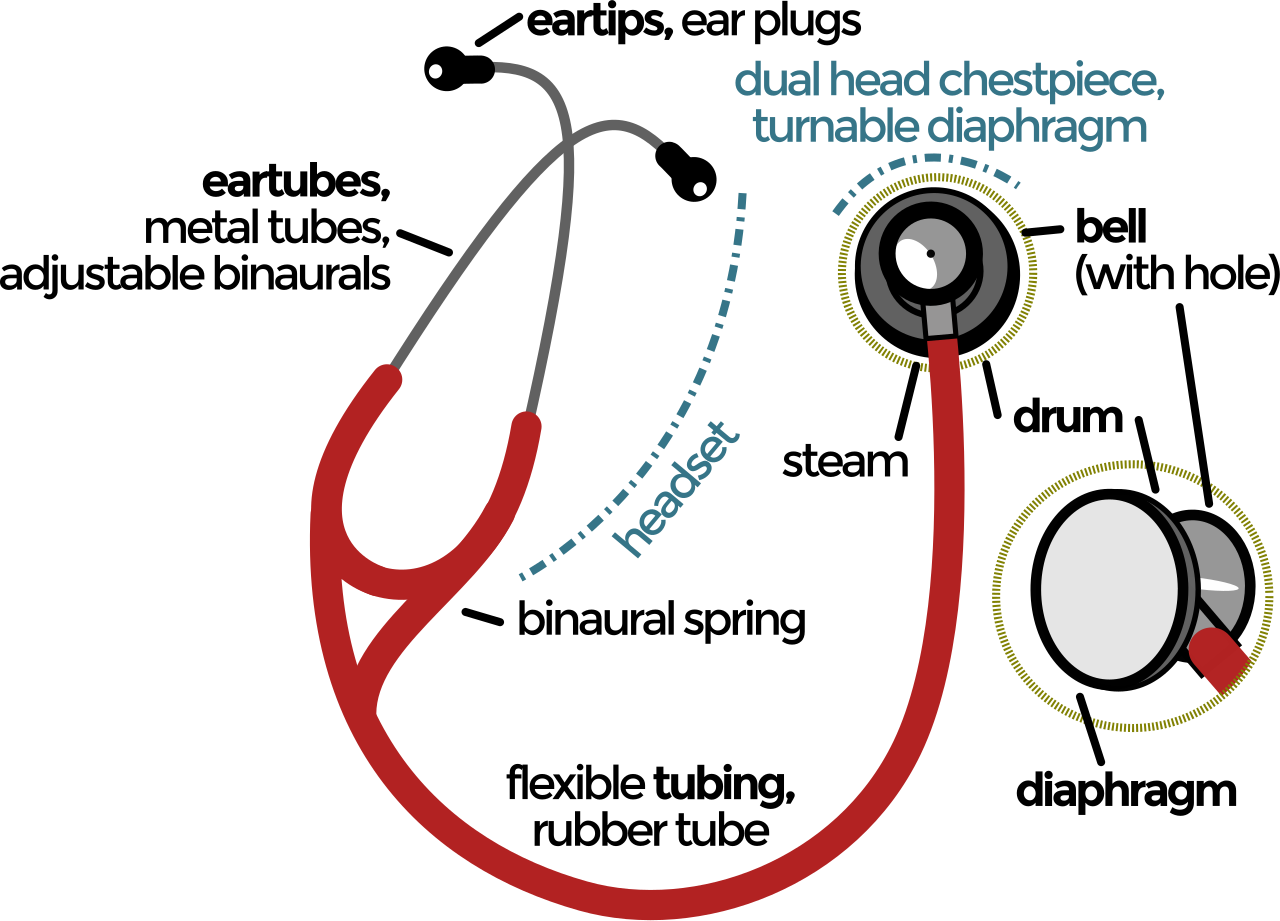
When it is time to listen closely, you rely on your stethoscope, which separates acoustic frequencies.
- The bell of the stethoscope is used to auscultate low-pitched bodily sounds. These low-pitched bodily sounds include heart murmurs and vascular bruits (the turbulent swoosh of blood flowing through a narrowed artery).
- The diaphragm of the stethoscope is used to auscultate high-pitched bodily sounds. High-pitched bodily sounds include normal breath sounds and normal bowel sounds.
The Neurological System
To evaluate a patient's level of consciousness, we use a universal metric. The Glasgow Coma Scale (GCS) evaluates eye opening, verbal response, and motor response.
Clinical Baseline: A Glasgow Coma Scale score of 15 indicates a fully alert and oriented patient. Conversely, a Glasgow Coma Scale score of 3 indicates deep coma or profound unresponsiveness.
When assessing cranial nerves, specifically the eyes, we use the acronym PERRLA, which stands for Pupils Equal, Round, Reactive to Light, and Accommodation. Shining a penlight into the patient's eye triggers the pupillary light reflex. This pupillary light reflex assesses the neurological function of the oculomotor nerve (Cranial Nerve III).

We must also assess motor pathways. Muscle strength is clinically graded on a standardized scale ranging from 0 to 5. A muscle strength grade of 5 indicates normal active movement against full manual resistance.
The Respiratory System
Lung auscultation requires knowing where to place your stethoscope and what sounds spell danger. Normal vesicular breath sounds are heard primarily over the peripheral lung fields—the soft, rustling sound of healthy air exchange.
When the airways are compromised, the acoustic signatures change dramatically:
- Respiratory wheezes indicate narrowed or obstructed airways, often heard in asthma or COPD.
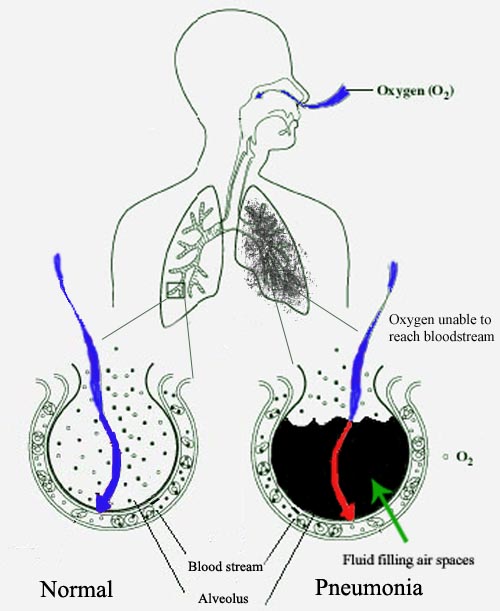
- Respiratory crackles indicate the presence of fluid or secretions in the alveoli or small airways, characteristic of heart failure or pneumonia.
- Stridor is a high-pitched respiratory sound indicating a severe upper airway obstruction. This is a medical emergency.
The Cardiovascular and Peripheral Systems
Cardiac assessment requires precise anatomical landmarks. The apical pulse is anatomically located at the fifth intercostal space at the left midclavicular line. This is where you hear the heartbeat most distinctly, yielding the classic "lub-dub."
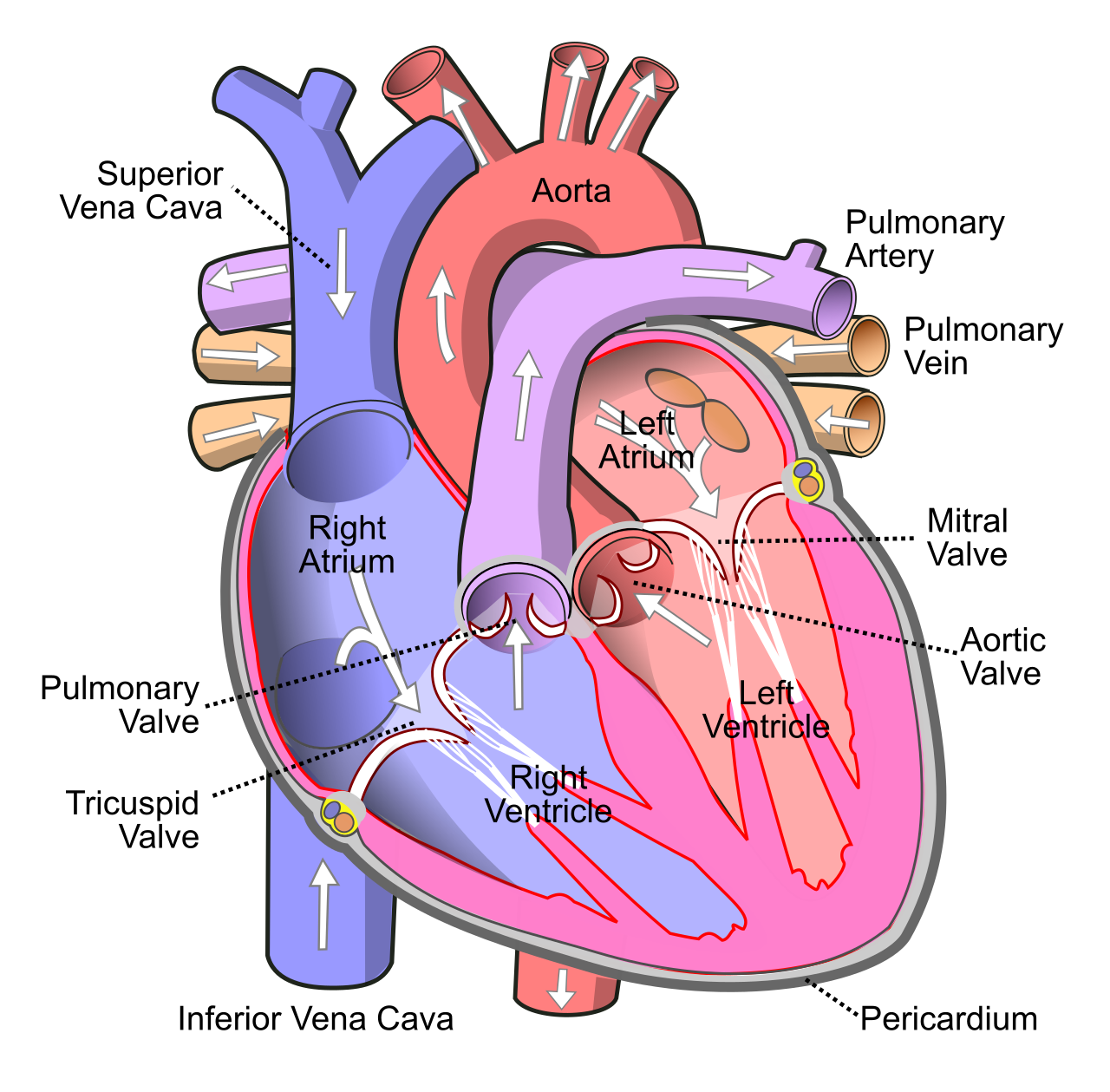
- The S1 heart sound ("lub") represents the closure of the atrioventricular valves. The atrioventricular valves include the mitral valve and the tricuspid valve.
- The S2 heart sound ("dub") represents the closure of the semilunar valves. The semilunar valves include the aortic valve and the pulmonic valve.
Perfusion extends to the very tips of the fingers. Capillary refill time is a clinical measurement used to assess peripheral blood perfusion. By pressing on the nail bed until it blanches and releasing, you time how quickly the pink color returns. A normal capillary refill time in a healthy adult is less than three seconds.
If perfusion is chronically poor, the body physically adapts. Clubbing of the fingernails—an abnormal rounding and swelling of the nail bed—suggests long-term chronic tissue hypoxia. Additionally, we check for fluid shifting into the interstitial spaces. Pitting edema is clinically graded on a standardized scale ranging from 1+ to 4+, depending on the depth and duration of the indentation left by your thumb.

The Gastrointestinal System and Hydration
Returning to the abdomen, you listen with the diaphragm of your stethoscope. Normal bowel sounds occur at an average rate of 5 to 30 times per minute. If you suspect a paralytic ileus, you must be patient: absent bowel sounds can only be medically confirmed after listening continuously for five minutes in each abdominal quadrant.
Hydration is intimately tied to GI fluid loss or poor intake. Skin turgor is assessed by pinching a fold of skin to evaluate the patient's hydration status. If the skin snaps back immediately, hydration is adequate. However, prolonged tenting of the skin during a turgor assessment strongly indicates clinical dehydration.
The Lymphatic System
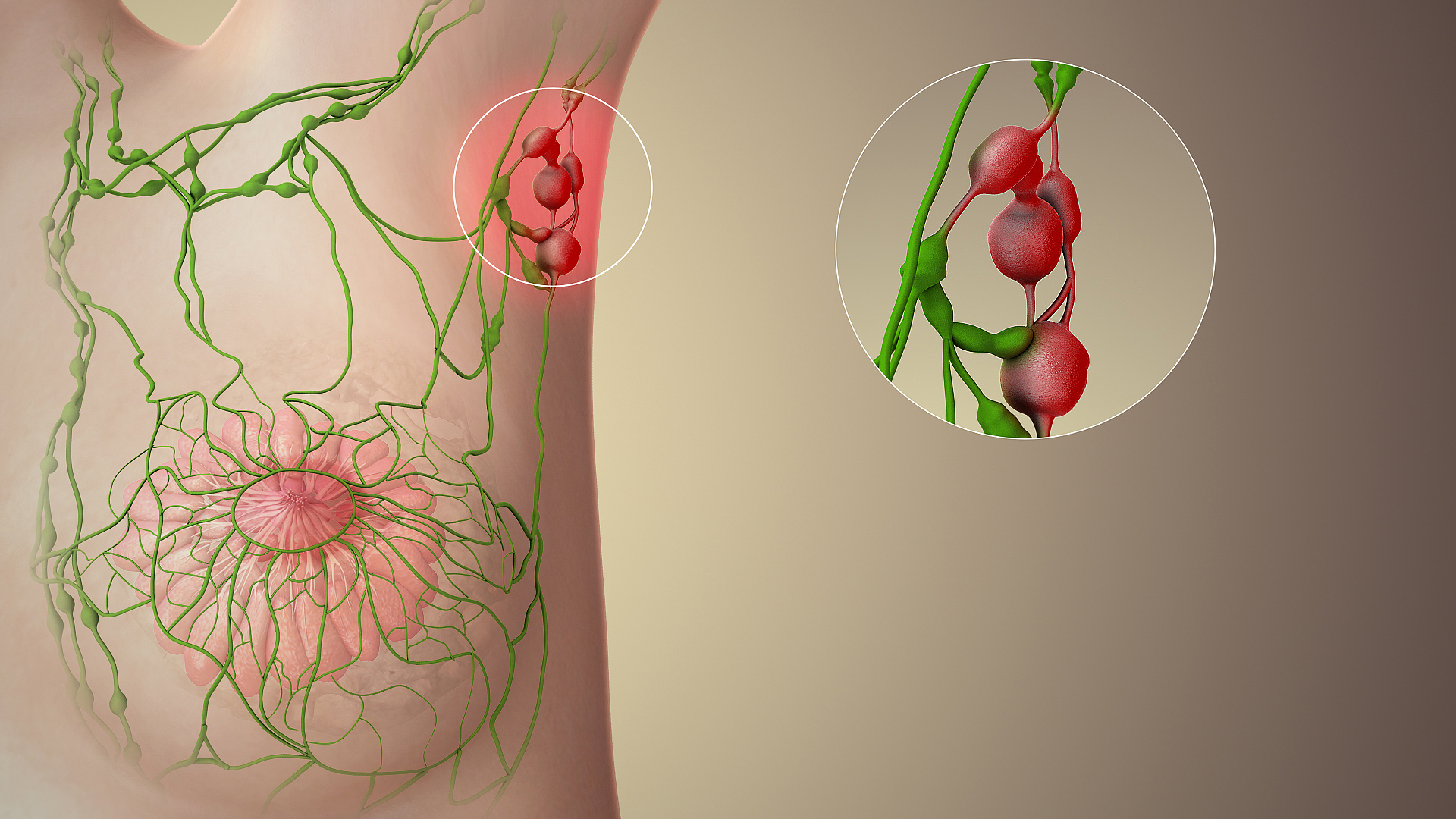
During palpation of the head and neck, you will evaluate lymph nodes. Their physical characteristics tell a vivid clinical story:
- Enlarged, tender, and highly mobile lymph nodes generally indicate an acute localized infection. The immune system is actively fighting a transient threat.
- Hard, fixed, and painless lymph nodes strongly suggest underlying malignancy. The node is trapped by invading neoplastic tissue.
Patients are not monolithic; anatomy and psychology shift from birth to old age.
Pediatrics
When dealing with an infant, standard hospital procedures can cause profound anxiety. Therefore, physical assessment of an infant must proceed from the least invasive procedures to the most invasive procedures to minimize distress. Watch their breathing and listen to their heart while they sleep or rest in a parent's arms, saving the uncomfortable checks (like examining the ears or throat) for last.
Growth metrics and cranial anatomy are unique to this population:
- The head circumference is routinely measured during physical assessments of children up to 36 months of age to ensure proper brain development.
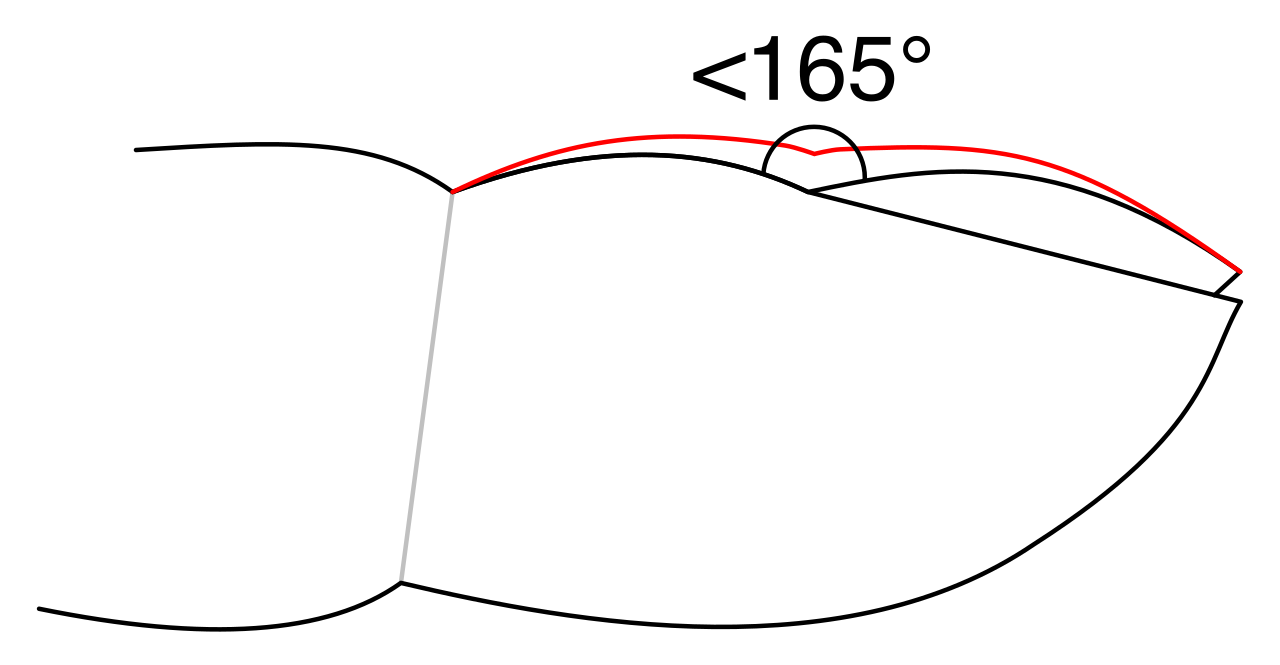
- The skull plates have not yet fused. The anterior fontanelle of an infant normally closes between 12 and 18 months of age.
- Because the fontanelle is an open window to the cranial vault, it acts as a pressure gauge. A severely sunken anterior fontanelle in an infant suggests severe dehydration. Conversely, a bulging anterior fontanelle in a resting infant suggests increased intracranial pressure.

Obstetrics
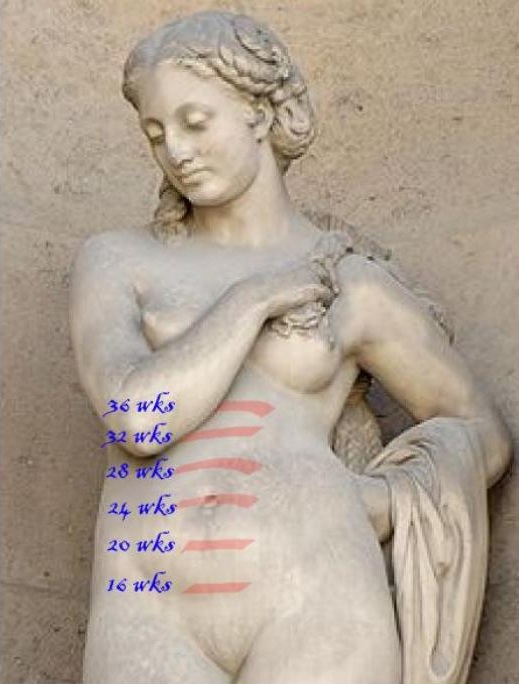
Maternal assessments require an understanding of two patients at once. The physical assessment of a pregnant woman includes measuring the fundal height to estimate fetal growth.
Positioning a pregnant patient requires acute clinical foresight. As the gravid uterus grows, it can compress the heavy vessels running along the spine when the mother lies flat. Placing a wedge under the right hip of a pregnant patient prevents supine hypotensive syndrome during a physical assessment, ensuring continuous venous return to the heart.
Geriatrics
The physiological wear and tear of time changes mobility. Geriatric patients often require extended time allowances for positional changes during a comprehensive physical assessment. Rushing a frail elderly patient risks falls, induces stress, and yields artificially elevated vital signs.
Your brilliant assessment is useless if it is not communicated accurately. The global gold standard for structured clinical handover is the SBAR communication framework, which stands for Situation, Background, Assessment, and Recommendation. The SBAR framework standardizes the verbal communication of physical assessment findings among the interprofessional healthcare team.
When calling a physician in the middle of the night regarding a deteriorating patient, strict adherence to this structure saves lives:
- Situation: Identifies the patient and the immediate clinical reason for the communication. ("Dr. Ahmed, I am calling about Mr. Ali in Room 4; his oxygen saturation has acutely dropped to 85%.")
- Background: The clinical context.
- Assessment: Includes the nurse's objective physical examination findings. ("I auscultated bilateral respiratory crackles and noted 3+ pitting edema in his lower extremities.")
- Recommendation: Communicates the nurse's suggested clinical action to the provider. ("I recommend ordering a stat chest X-ray and evaluating him for an IV diuretic.")
Finally, when committing your findings to the medical record, efficiency is paramount. Many modern Saudi hospitals utilize charting by exception, a documentation method that records only physical assessment findings that deviate from defined normal limits. This method reduces charting redundancy while instantly highlighting the critical abnormalities that demand the medical team's immediate attention.