Community Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Imagine standing at the mouth of a rushing river, pulling drowning people from the water one by one. Acute care nursing is the vital act of resuscitation on the riverbank, but community nursing requires walking upstream to find out who is pushing them in, or why the bridge collapsed in the first place. Rather than waiting for pathology to manifest within the isolated walls of a hospital room, community nursing focuses on promoting health and preventing disease across entire populations. This discipline demands a shift in perspective—from treating the singular patient in bed four to diagnosing and treating the collective socio-environmental ecosystem.
To pass the Saudi Nursing Licensure Examination (SNLE) and practice effectively within the Kingdom, you must understand how to navigate this ecosystem. The hospital is only one small node in a vast network of human health. We must examine how diseases move, how populations behave, and how nurses engineer systemic change.
Healthcare in Saudi Arabia is undergoing a profound structural evolution. Historically, health systems globally have been reactive, heavily weighting resources toward hospitals. However, the Saudi Vision 2030 Health Sector Transformation Program prioritizes preventive public health initiatives over hospital-based curative care.
Why build a massive tertiary center to treat end-stage renal disease if we can intervene decades earlier? To achieve this, Saudi Arabia's Vision 2030 Health Sector Transformation Program prioritizes expanding public access to primary healthcare centers. By decentralizing care, nurses are positioned at the community level, catching risk factors before they become irreversible pathologies. Furthermore, nurses are no longer just bedside caregivers; they are systems architects. Recognizing this, the Saudi Patient Safety Center developed competency frameworks empowering nurses to lead national quality improvement initiatives, ensuring that those closest to the community are designing its safety protocols.
Before intervening, a nurse must assess. Just as you auscultate a patient's lungs, a community health assessment identifies the collective health needs of a specific geographic population.
This begins with direct, grounded observation. Often, community health nurses conduct windshield surveys by directly observing neighborhood infrastructure from a moving vehicle. This is not a deep statistical dive; rather, a windshield survey provides an initial subjective assessment of a community's environmental health risks. From the car, you observe: Are there safe sidewalks for exercise? Are local grocery stores stocking fresh produce, or only heavily processed foods? Is there visible industrial smog?
Once you identify the risks, you must collaborate to solve them. Cooperative decision-making in community health requires engaging local community members in identifying public health priorities. You cannot force a health program on a neighborhood. Lasting change requires community partnerships, which involve collaborative relationships between healthcare providers and local civic organizations. Ultimately, community partnerships maximize available health resources by sharing accountability for public health outcomes.
Through these partnerships, the ultimate goal is achieved: community empowerment, which occurs when a specific population gains control over the socioeconomic factors influencing their health outcomes. When a neighborhood advocates for and secures its own clean water or safe parks, it has been truly empowered.
To manage a population's health, you must understand how disease propagates. We visualize this using the epidemiological triangle model, which analyzes disease transmission through the interactions of an infectious agent, a susceptible host, and a supportive environment. Break any side of this triangle, and you stop the disease.
Consider a real-world priority in the Kingdom: Middle East Respiratory Syndrome Coronavirus (MERS-CoV), which is a zoonotic viral illness endemic to Saudi Arabia.
- The Environment & Agent: The virus circulates in specific agricultural environments. Specifically, dromedary camels are the primary animal reservoir for Middle East Respiratory Syndrome Coronavirus transmission to humans.
- The Susceptible Host: Not everyone infected experiences the same outcome. Individuals with diabetes mellitus face a significantly higher risk for severe complications from Middle East Respiratory Syndrome Coronavirus, demonstrating how a pre-existing non-communicable disease (NCD) alters host susceptibility to an infectious agent.

To track these variables, the Ministry of Health relies on robust data. The Health Electronic Surveillance Network is the official public health disease reporting and tracking system in Saudi Arabia. Nurses feed data into this system, which measures disease spread using two critical metrics:
Incidence vs. Prevalence Think of a bathtub.
- Incidence rate measures the number of newly diagnosed cases of a disease within a specific population during a defined time period. (The water flowing from the faucet into the tub).
- Prevalence rate measures the total number of existing disease cases within a specific population at a given point in time. (The total volume of water currently sitting in the tub).
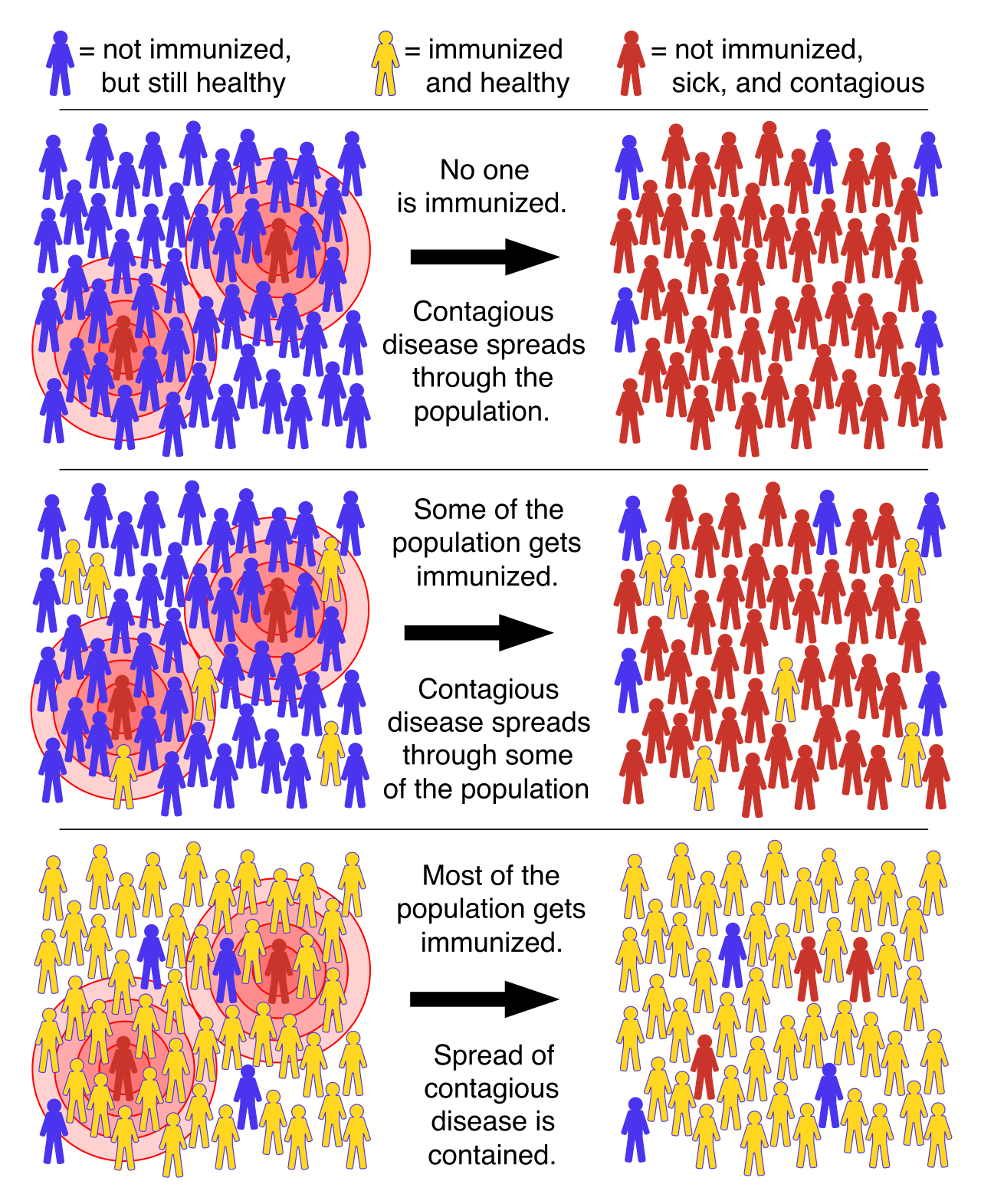
For vaccine-preventable diseases, we manipulate these rates through immunization. The goal is the creation of a biological shield: herd immunity occurs when a large portion of a community becomes immune to a specific infectious disease. When the virus cannot find a susceptible host, transmission chains break. Therefore, high levels of herd immunity significantly reduce the disease transmission risk for unvaccinated individuals (such as newborns or immunocompromised oncology patients).
We classify nursing interventions based on when they occur in the timeline of a disease. Master this framework, as it dictates clinical decision-making on the ward and in the clinic.
| Level of Prevention | Core Definition | Real-World Application |
|---|---|---|
| Primary Prevention | Primary prevention strategies aim to prevent the initial occurrence of a disease. | Intervening before pathology exists. Administering routine vaccinations is an example of primary disease prevention, as it stops the infectious agent from ever taking hold. |
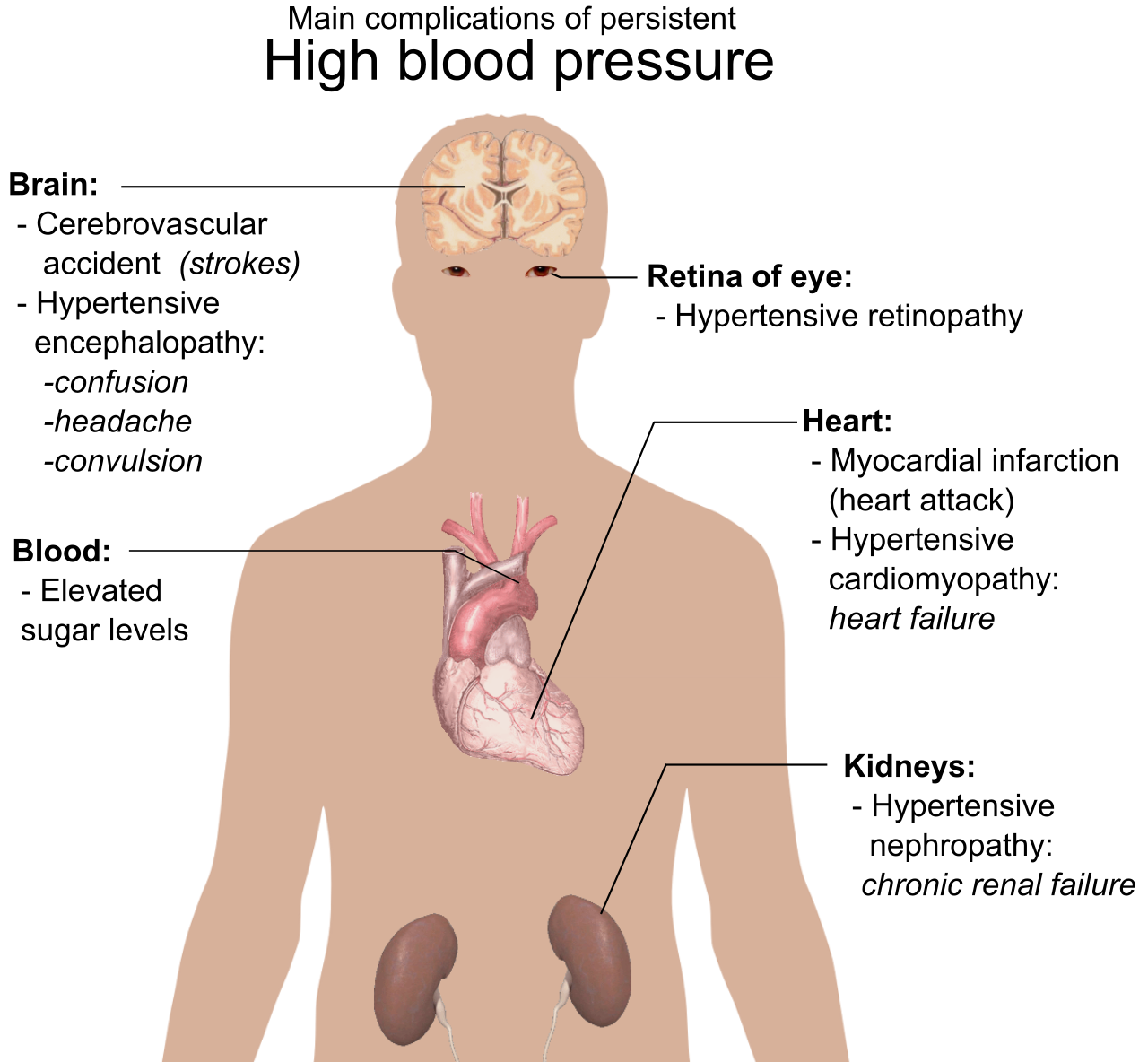
| Secondary Prevention | Secondary prevention involves early detection and prompt treatment of an existing asymptomatic disease. | Catching a silent killer early. In KSA, hypertension is a major public health burden requiring extensive community screening initiatives throughout Saudi Arabia. Consequently, community screening programs for hypertension are classified as secondary prevention. |
| Tertiary Prevention | Tertiary prevention focuses on rehabilitation and minimizing the long-term complications of an established chronic illness. | Mitigating damage when the disease is already present and permanent. Establishing a diabetic foot care clinic is a form of tertiary disease prevention, preventing ulcers from progressing to amputations. |
You can build the best clinics in the world, but if patients do not understand their disease, outcomes will fail. The high prevalence of diabetes mellitus in Saudi Arabia necessitates targeted community-wide lifestyle education on nutrition.
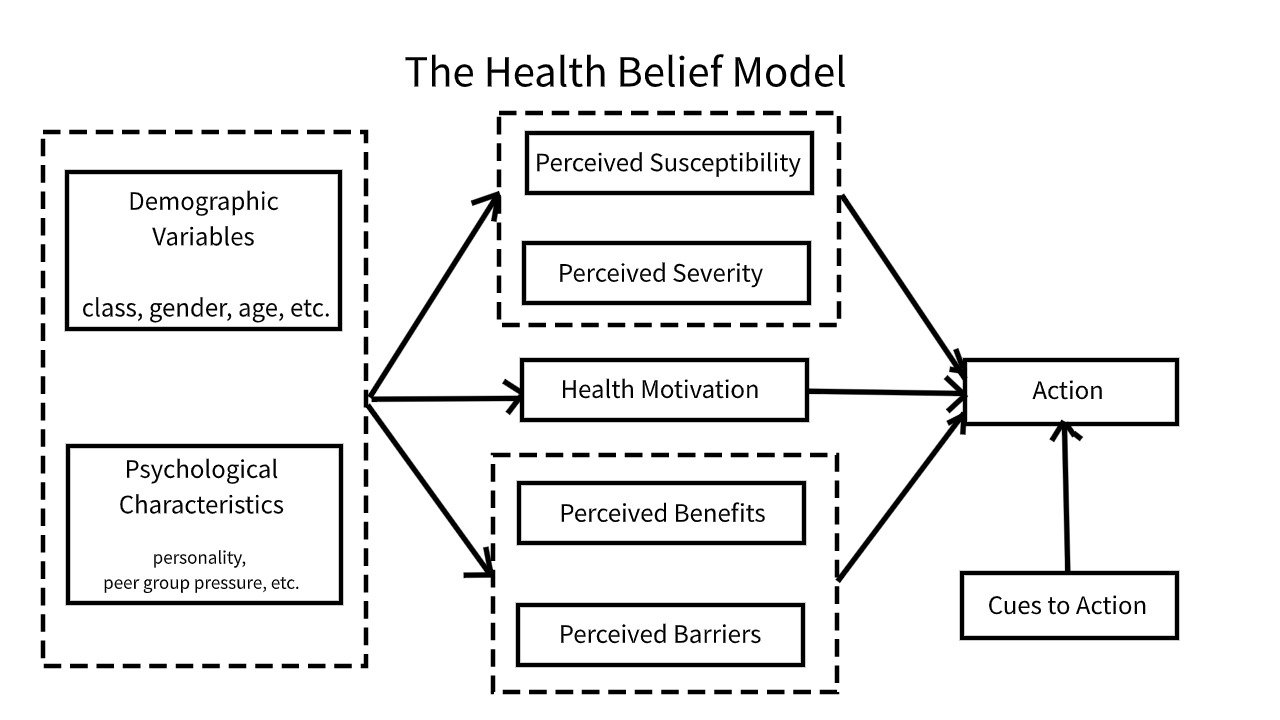
But how do we effectively teach? We must first look through the lens of the Health Belief Model, which predicts a patient's engagement in health-promoting behaviors based on the patient's perceived susceptibility to an illness. If a patient does not truly believe that a high-carbohydrate diet will lead to blindness or renal failure (perceived susceptibility and severity), they will not adopt preventive behaviors.
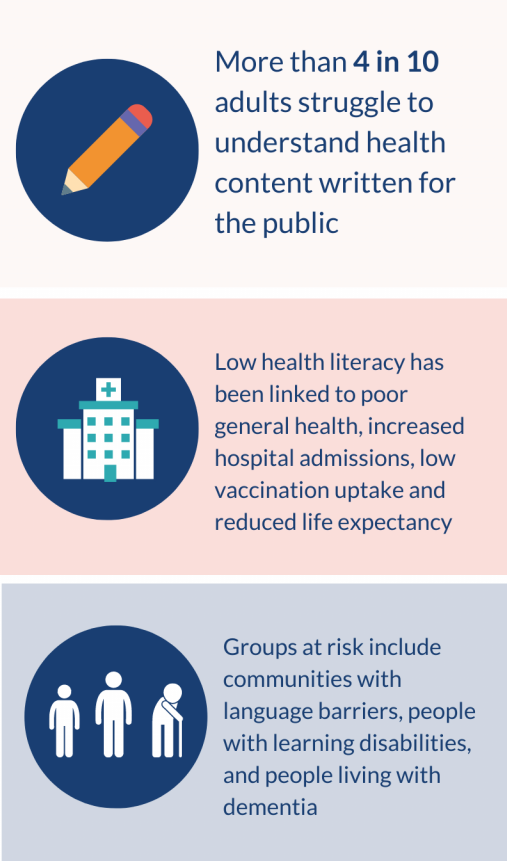
Before handing a patient a dietary pamphlet, you must know if they can comprehend it. Effective community health education requires an initial assessment of the target audience's baseline health literacy. This is critical because low health literacy limits a patient's ability to successfully navigate complex healthcare systems (like booking follow-up appointments or understanding pharmacy labels). More alarmingly, low health literacy decreases patient compliance with prescribed chronic disease management plans, directly driving up hospital readmissions.
When delivering this education, format matters. Sitting a patient down for a one-way lecture is highly inefficient. Instead, group health education sessions yield higher knowledge retention rates when incorporating interactive peer discussions. When diabetic patients in a community center share their own culturally relevant cooking substitutions with one another, the knowledge sticks.
Speaking of culture: Culturally competent community nursing integrates local family dynamics into individual care plans. In Saudi Arabia, healthcare decisions are rarely made in isolation by the individual; they are family affairs. A discharge plan that ignores the matriarch or patriarch of the family is a plan destined to fail.
Community nursing extends into specialized micro-populations, targeting individuals exactly where they live, work, and learn.
School Nursing
A child cannot learn if they are unwell. Beyond simply distributing ice packs, school nursing interventions aim to reduce student absenteeism through localized health promotion (such as asthma management or hand hygiene campaigns). On a macro level, school nurses manage population health by tracking student immunization compliance, acting as the frontline defense against outbreaks of measles or pertussis.
Occupational Health Nursing
Adults spend the majority of their waking hours at work. Occupational health nursing focuses on preventing workplace injuries. In a rapidly industrializing economy, this is vital. For example, in petrochemical plants or manufacturing facilities, occupational health nurses assess industrial environments to reduce employee exposure to chemical hazards, implementing primary prevention right on the factory floor.

Home Healthcare Nursing
The boundaries of the hospital are expanding. Home healthcare nursing provides chronic disease management outside the acute hospital setting, reducing inpatient overcrowding. Furthermore, it brings profound dignity to the end of life, as home healthcare nursing facilitates palliative care interventions directly within a patient's private residence, allowing patients to remain surrounded by their families.
Vulnerable Populations
Finally, a community is only as healthy as its most marginalized members. Vulnerable populations experience disproportionate morbidity rates due to systemic barriers limiting healthcare access. Whether due to socioeconomic status, geographic isolation, or disability, these groups face a steeper uphill battle to wellness. Community nurses advocate for vulnerable populations by connecting marginalized individuals with available social support resources, bridging the gap between clinical need and social infrastructure.