Gynecology
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
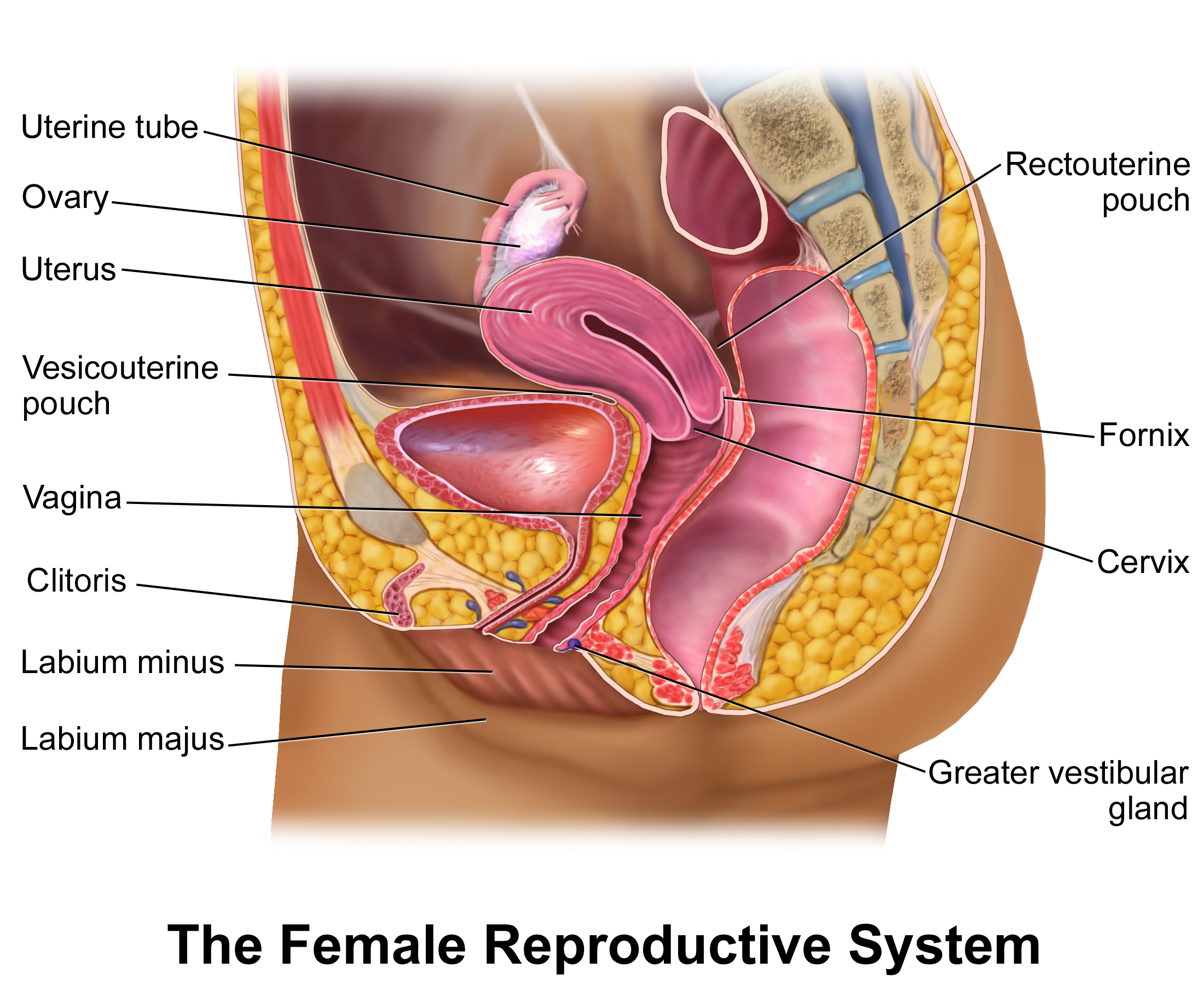
The female reproductive system operates on a precise, rhythmic feedback loop of hormones, cellular proliferation, and structural adaptation. Yet, clinical gynecology requires more than a mere mechanical understanding of this system; it demands an integration of physiological science with profound human sensitivity. For the nurse practicing in Saudi Arabia, mastering this domain means bridging evidence-based screening, infection control, and oncological care with stringent cultural and regulatory frameworks. We are not just observing tissues under a microscope; we are navigating the deeply personal intersection of patient dignity, family dynamics, and institutional safety standards.
Before we touch a patient, we must understand the environment of trust we are operating within. In Saudi Arabia, gynecological care is built upon a foundation of cultural respect and strict legal guidelines overseen by the Saudi Commission for Health Specialties (SCFHS).
Because Islamic principles require healthcare providers to respect a female patient's modesty during gynecological examinations, we must meticulously manage physical exposure, ensuring the patient remains draped and comfortable. This is not merely a courtesy; it is a clinical standard. If the examination is performed by a male practitioner, the presence of a female chaperone is mandated. This protects the patient's dignity and provides institutional liability protection.
Additionally, the Saudi Commission for Health Specialties requires documented informed consent prior to any invasive gynecological procedure. The patient must understand exactly what the procedure entails, the risks, and the alternatives before we proceed. We must also rigorously protect the patient's data; healthcare providers must maintain strict confidentiality regarding a patient's sexually transmitted infection (STI) status, as unauthorized disclosure carries profound social and legal consequences.
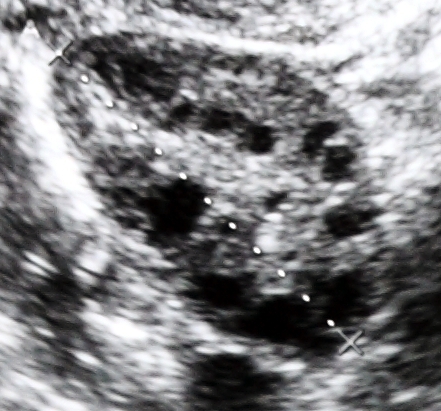
When evaluating an unmarried woman, our approach fundamentally shifts. A virginity-preserving approach to pelvic examinations is culturally preferred for unmarried women in Saudi Arabia unless medically necessary. Because of cultural norms regarding hymen integrity, transvaginal ultrasounds are generally avoided in unmarried women who are not sexually active. Instead, we rely on transabdominal ultrasounds—requiring the patient to have a full bladder to create an acoustic window—to visualize the pelvic organs.
When we do need to assess the female reproductive organs, we rely on a specific toolkit of diagnostics.
A bimanual pelvic examination is performed to manually assess the size and mobility of the uterus and ovaries. By placing two fingers in the vagina and pressing down on the lower abdomen with the other hand, the clinician can "trap" the organs between their hands, checking for masses or immobility indicative of adhesions.
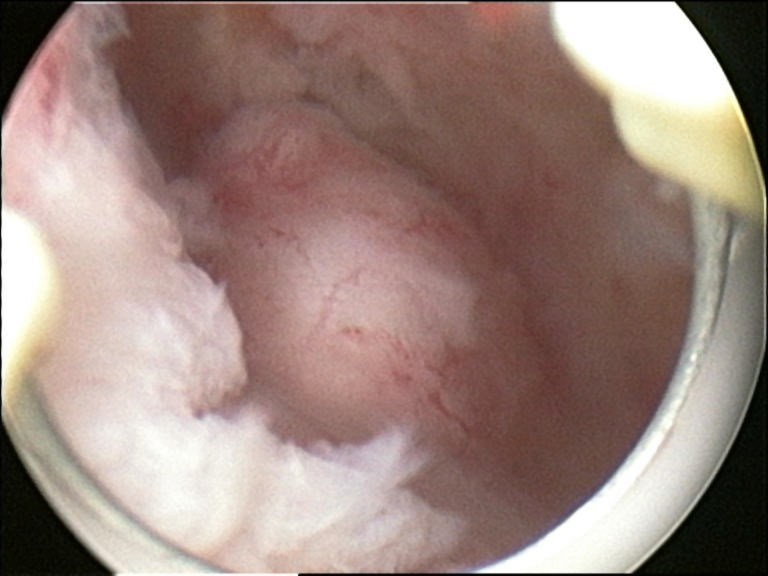
If we are looking for precancerous cells, a colposcopy provides a magnified visual examination of the cervix to detect precancerous lesions. During this procedure, acetic acid is applied directly to the cervix during a colposcopy to highlight areas of abnormal cell growth—the abnormal, rapidly dividing cells uptake the acid and turn stark white, guiding the provider's biopsy.
When we need to look inside the uterus, a hysteroscopy permits direct visual inspection of the internal uterine cavity using a specialized endoscope, allowing us to identify polyps, fibroids, or structural anomalies.
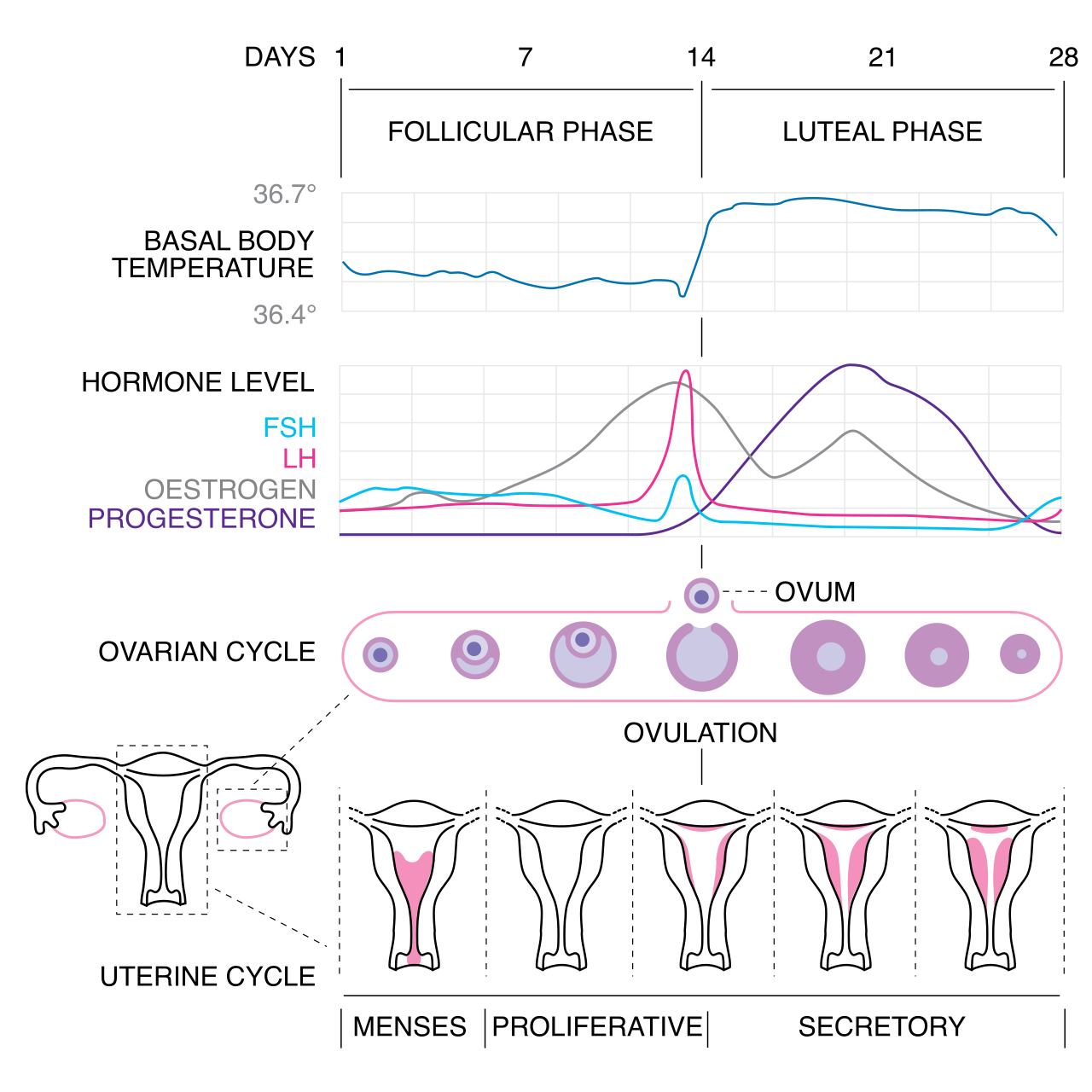
The menstrual cycle is a hormonal symphony. When the timing is off, we must look for the underlying physiological short-circuit.
- Primary amenorrhea is the absence of menarche by age 15 in the presence of normal secondary sexual characteristics. Here, the hormonal sequence simply hasn't started.
- Secondary amenorrhea is the cessation of regular menses for three months or irregular menses for six months. The rule of thumb in nursing? Always rule out the most obvious answer first: pregnancy is the most common cause of secondary amenorrhea.
When menstruation is occurring but agonizingly painful, we call it dysmenorrhea, which is characterized by painful uterine cramping during menstruation. This cramping is driven by prostaglandins, which cause the uterine muscle to aggressively contract and temporarily cut off its own blood supply (ischemia). Knowing this mechanism tells us exactly how to treat it: nonsteroidal anti-inflammatory drugs (NSAIDs) relieve dysmenorrhea by inhibiting prostaglandin synthesis.
When Endometrium Goes Rogue: Endometriosis
Endometriosis involves the growth of endometrial tissue outside the uterine cavity. Think about what endometrial tissue does: it responds to hormones by thickening, and then it bleeds. Therefore, ectopic endometrial tissue bleeds cyclically during menstruation.
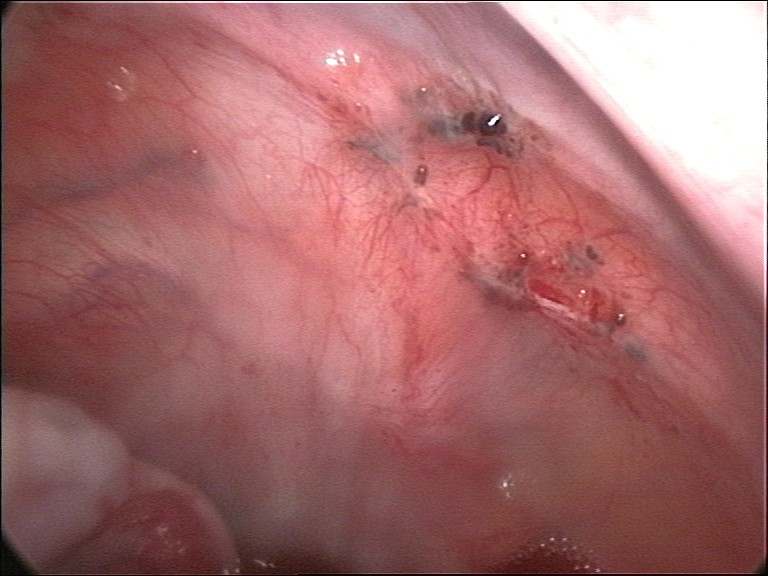
However, unlike normal menstrual blood which exits through the vagina, this blood has nowhere to go. Internal bleeding from endometriosis causes pelvic inflammation. Over months and years, this chronic pelvic inflammation from endometriosis frequently leads to structural adhesions—literally gluing pelvic organs together and causing severe, chronic pain.
Polycystic Ovary Syndrome (PCOS)
PCOS is a complex metabolic and endocrine disorder. It is fundamentally characterized by hyperandrogenism (excess male hormones, leading to hirsutism and acne) and it causes chronic ovulatory dysfunction (irregular or absent periods).
But the engine driving this disorder is often metabolic: insulin resistance is a central pathophysiological feature of polycystic ovary syndrome. The body pumps out excess insulin, which in turn stimulates the ovaries to produce more androgens. This is why a diabetes drug, Metformin, is often prescribed to patients with polycystic ovary syndrome to improve insulin sensitivity, thereby lowering insulin levels, decreasing androgen production, and helping restore ovulation.
We must distinguish between lower reproductive tract infections (vaginitis) and dangerous upper reproductive tract infections.
Vaginal Infections (Vaginitis)
Different organisms create distinct, highly recognizable clinical pictures. Learn to recognize these instantly on the ward:
| Condition | Pathogen Type | Key Clinical Presentation & Diagnosis | Treatment Considerations |
|---|---|---|---|
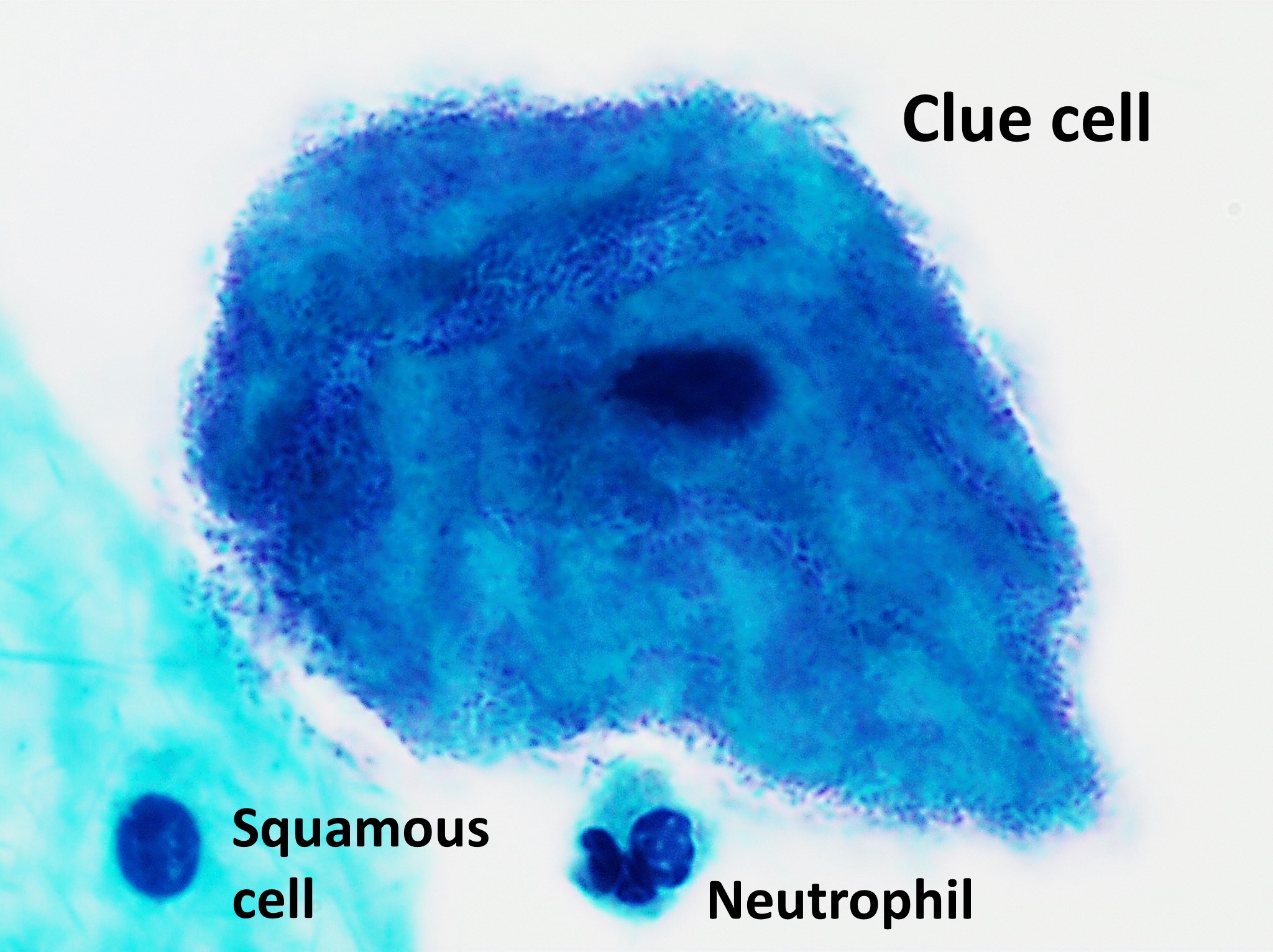
| Bacterial Vaginosis (BV) | Bacterial Imbalance | Characterized by a thin vaginal discharge with a distinctive fishy odor. The presence of clue cells under microscopic examination confirms a diagnosis of bacterial vaginosis. | Metronidazole or Clindamycin. |
| Vulvovaginal Candidiasis | Fungal (Yeast) | Typically causes a thick vaginal discharge resembling cottage cheese and intense pruritus (itching). | Antifungals (e.g., Fluconazole). |
| Trichomoniasis | Parasite (Protozoa) | Trichomonas vaginalis infection presents with a yellow-green frothy vaginal discharge. | Metronidazole is the primary pharmacological treatment for Trichomonas vaginalis infections. |

Critical Safety Warning: Patients taking metronidazole must abstain completely from alcohol consumption to prevent a severe disulfiram-like reaction. This interaction blocks the breakdown of alcohol, leading to a massive buildup of acetaldehyde, causing violent nausea, vomiting, flushing, and tachycardia.
Pelvic Inflammatory Disease (PID)
Think of the female reproductive tract as an open highway from the outside world directly into the peritoneal cavity. Pelvic inflammatory disease is an ascending infection of the upper female reproductive tract. The pathogens start in the cervix and travel upward.
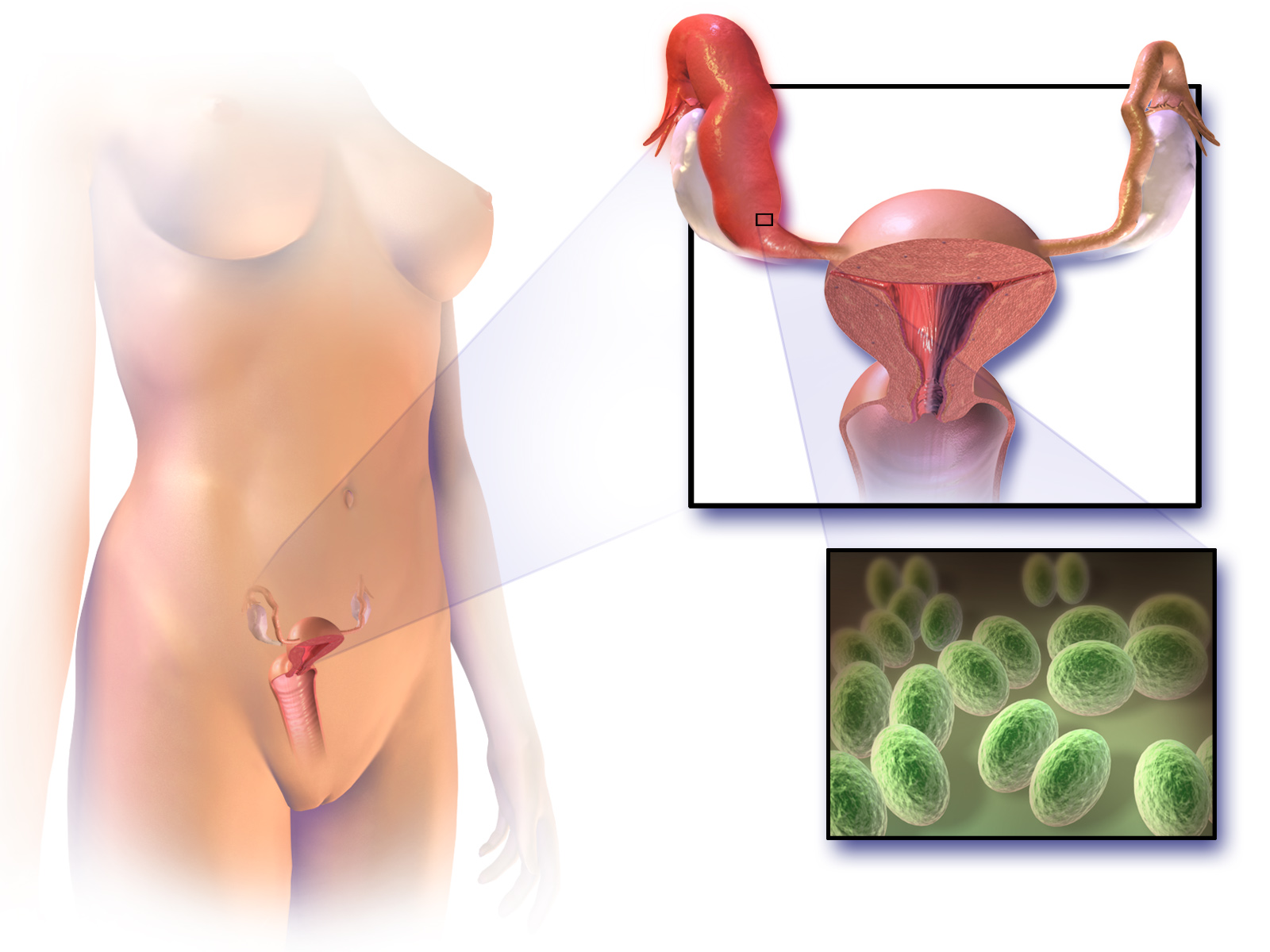
Chlamydia trachomatis is a primary causative organism of pelvic inflammatory disease, and Neisseria gonorrhoeae is a frequent bacterial cause.
Why do we treat PID so aggressively? Because of the aftermath. Untreated pelvic inflammatory disease dramatically increases the risk of an ectopic pregnancy. Furthermore, the fallopian tube scarring from pelvic inflammatory disease increases the risk of infertility. The delicate cilia in the tubes get destroyed, trapping fertilized eggs or preventing sperm from reaching the egg entirely.
The pelvic floor is a muscular sling supporting the bladder, uterus, and rectum. When this sling weakens—often due to childbirth or aging—organs can prolapse (fall) out of place.
- A cystocele occurs when the urinary bladder prolapses into the anterior vaginal wall. Because the bladder's angle is compromised, a cystocele frequently leads to stress urinary incontinence (leaking urine when coughing or laughing).
- A rectocele involves the prolapse of the rectum into the posterior vaginal wall, often causing difficulty with bowel movements.

To combat this, we teach patients to perform Kegel exercises, which strengthen the pelvic floor musculature. Clinically, strong pelvic floor muscles help manage the symptoms of mild pelvic organ prolapse without the immediate need for surgical intervention.
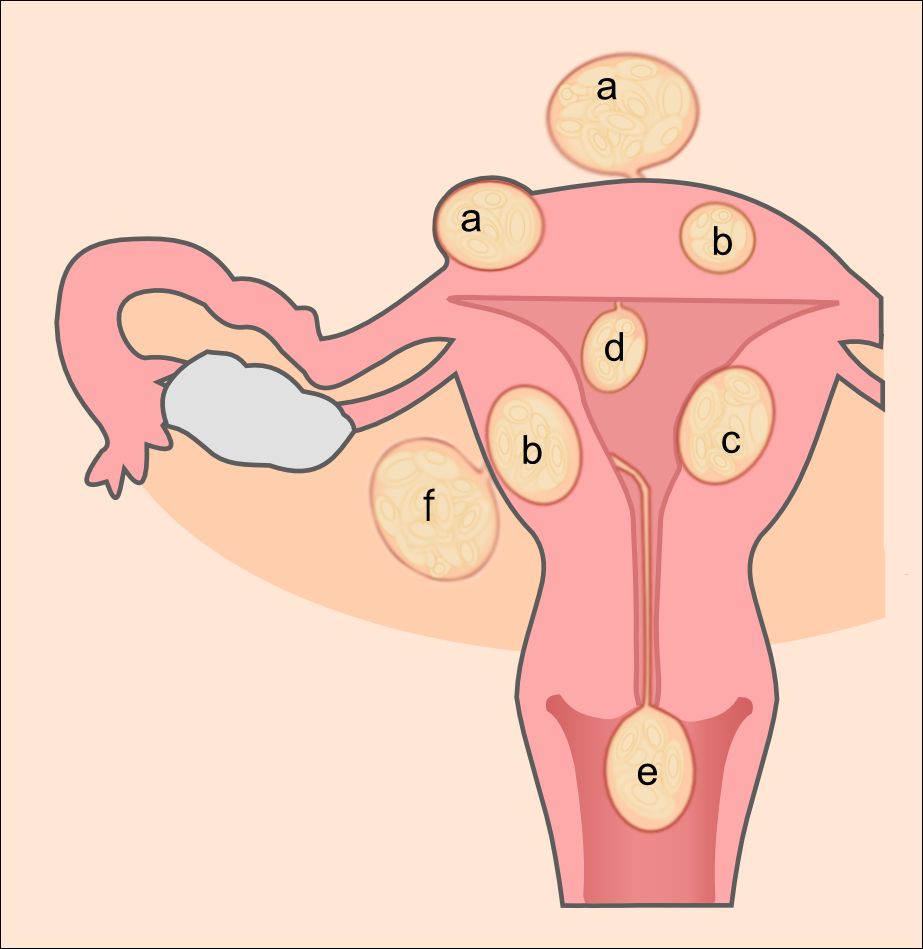
Uterine Fibroids
Uterine leiomyomas are benign smooth muscle tumors of the uterus. You will almost never hear them called that on the floor; uterine leiomyomas are commonly referred to as fibroids in clinical practice. Because they enlarge the surface area of the uterine lining and disrupt normal uterine contractions, heavy menstrual bleeding is the most common presenting symptom of uterine fibroids, often leading to profound anemia.
Cancer care requires vigilant screening, as early symptoms are often easily ignored by patients.
Cervical Cancer: This is a virus-driven malignancy. Human papillomavirus types 16 and 18 are responsible for the majority of cervical cancer cases.
Endometrial Cancer: This affects the lining of the uterus. Unexplained postmenopausal bleeding is the classic presenting symptom of endometrial cancer. Any woman bleeding after menopause needs immediate investigation. An endometrial biopsy is the definitive diagnostic procedure for confirming endometrial cancer.
Ovarian Cancer: This is often called the "silent killer." Ovarian cancer is typically diagnosed in advanced stages due to the presence of vague early symptoms. The ovaries are deep in the abdomen, allowing tumors to grow quite large before causing distress. However, persistent abdominal bloating is recognized as a common early symptom of ovarian cancer.
Breast Cancer & Genetic Risk: BRCA1 and BRCA2 genetic mutations significantly increase the lifetime risk of developing breast and ovarian cancers. When a patient undergoes surgical intervention for severe breast cancer, they may require a radical mastectomy, which involves the complete removal of breast tissue alongside axillary lymph nodes and pectoral muscles.
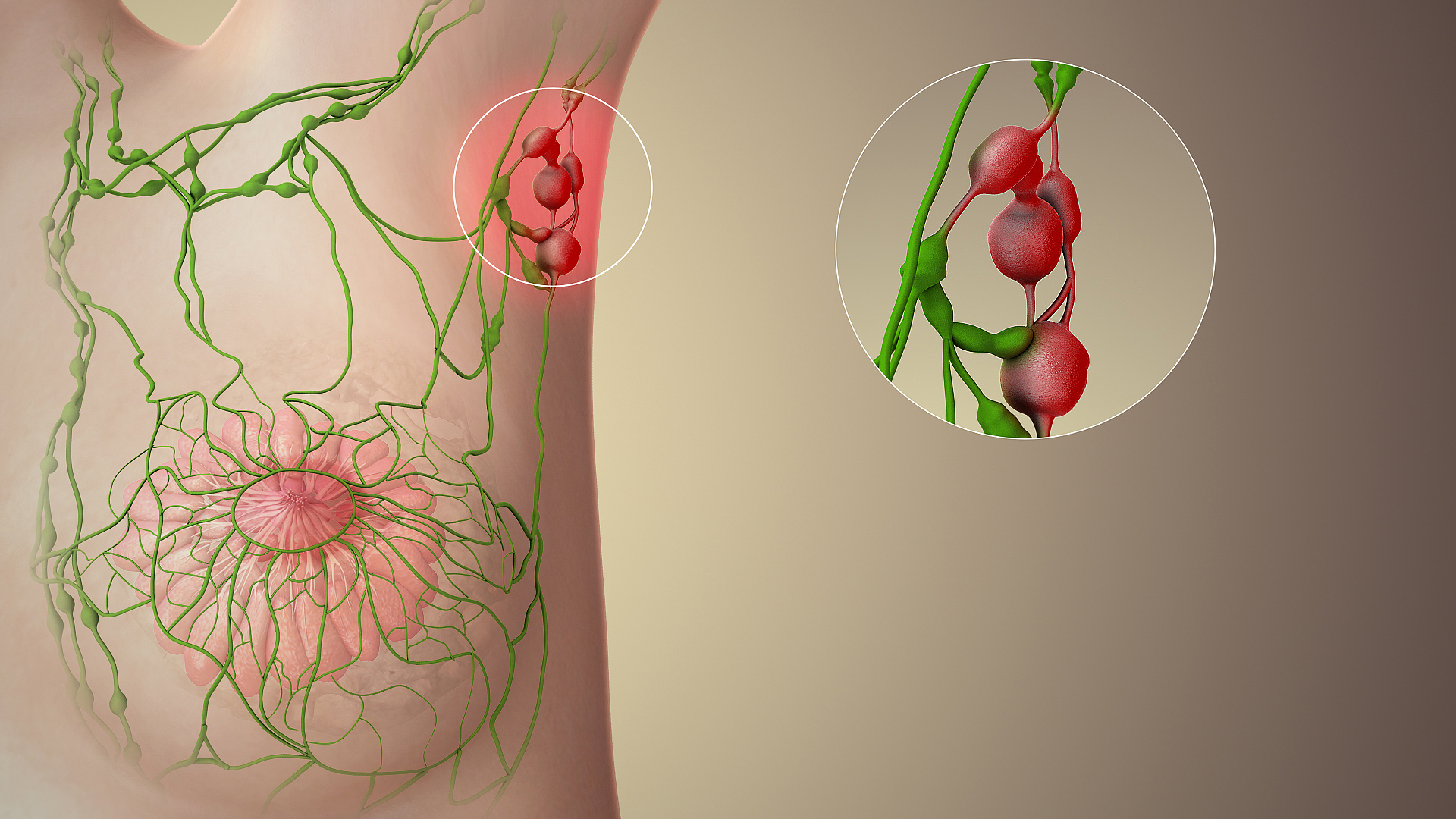
Patient Safety Imperative: Patients who undergo axillary lymph node dissection are at a high risk for developing lymphedema in the affected arm, as the lymphatic drainage pathway has been severed. Therefore, blood pressure measurements must never be taken on the arm located on the same side as a previous mastectomy. Doing so can trigger massive, irreversible arm swelling.
To catch these oncological threats early, we rely on established screening regimens.
- Cervical Screening: A Papanicolaou (Pap) smear is used as the primary screening tool for cervical cancer. Current clinical guidelines recommend starting cervical cancer screening at age 21 for sexually active women. To prevent the disease entirely, the human papillomavirus (HPV) vaccine is most effective when administered prior to initial sexual exposure.

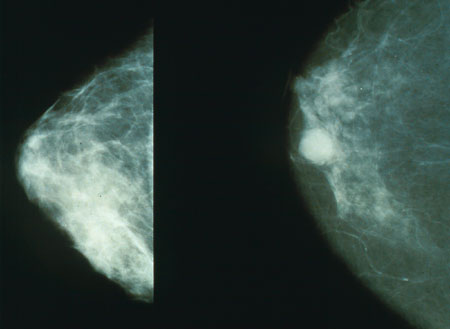
- Breast Screening: Annual mammography screening for breast cancer is typically recommended starting at age 40. We also encourage patients to know their own bodies; breast self-examinations are optimally performed five to seven days after the start of menstruation, when hormonal stimulation is lowest and the breasts are least tender and swollen.
The Menopausal Transition
As women enter menopause, estrogen levels plummet. This has multiple physiological effects. In the breasts, the decrease in estrogen levels after menopause reduces breast tissue nodularity, making screening easier.
However, in the skeletal system, the lack of estrogen accelerates bone resorption. Postmenopausal women require adequate calcium intake to prevent osteoporosis. Additionally, weight-bearing exercises help prevent bone density loss in postmenopausal women by forcing the bones to adapt to physical stress, thereby stimulating bone-building osteoblasts.

Contraception works either by altering the hormonal environment to prevent an egg from dropping, or by creating a hostile physical environment for sperm.
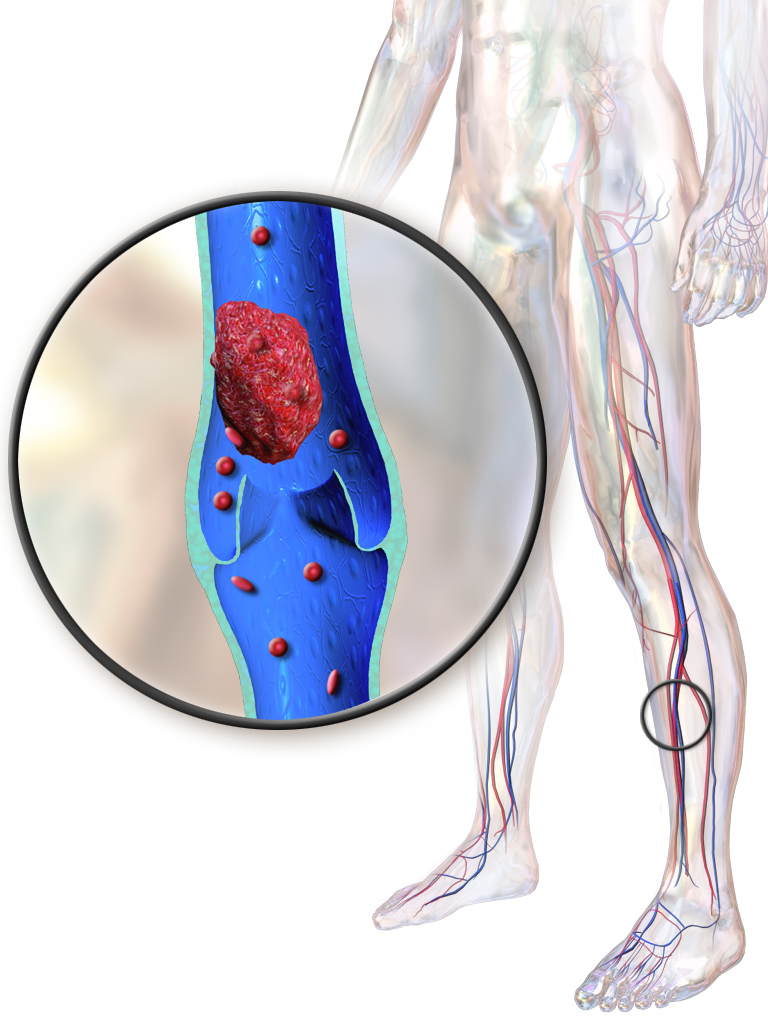
Hormonal Contraceptives: Combined oral contraceptives suppress ovulation by inhibiting the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the anterior pituitary. Without the LH surge, ovulation cannot occur. However, these drugs carry vascular risks. Estrogen-containing contraceptives increase a patient's risk of developing deep vein thrombosis (DVT) by increasing clotting factors in the blood. Heavy smoking while taking estrogen-containing contraceptives drastically elevates cardiovascular complication risks, including myocardial infarction and stroke.
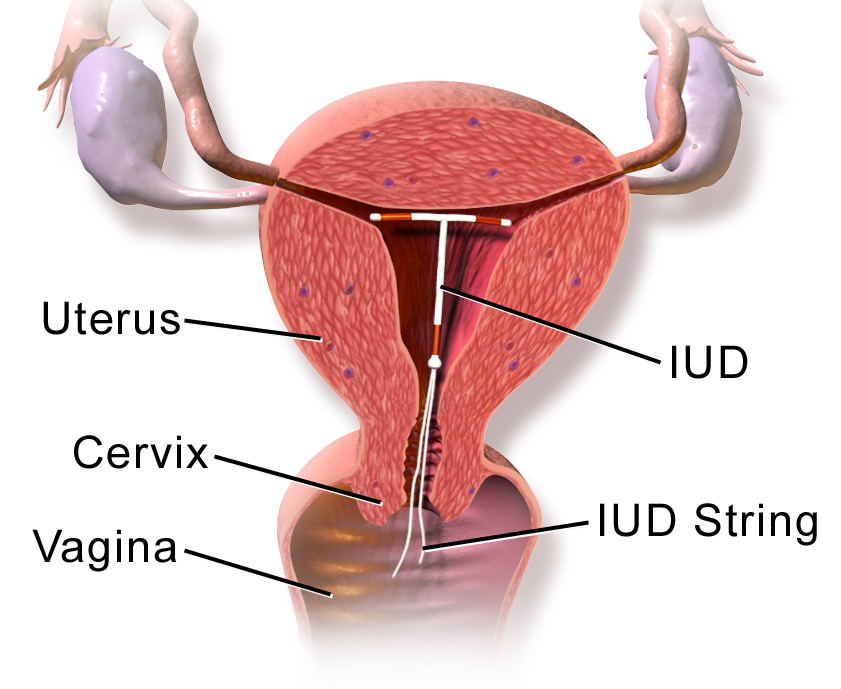
Intrauterine Devices (IUDs): Intrauterine devices are available in both hormonal and non-hormonal variations, and they work differently.
- A copper intrauterine device functions primarily as a spermicide by releasing copper ions into the uterine cavity, creating a highly toxic environment for sperm.
- The hormonal intrauterine device releases progestin locally, which thickens cervical mucus to create a physical barrier against sperm penetration and thins the uterine lining.
Barrier Methods: A diaphragm is a flexible cup placed over the cervix. Crucially, diaphragm use requires the concurrent application of spermicidal jelly to ensure maximum contraceptive efficacy. It is not just a physical wall; it is a vehicle to hold spermicide directly against the cervix. Furthermore, a diaphragm must remain in the vaginal canal for at least six hours following sexual intercourse to ensure any surviving sperm have perished before the barrier is removed.
