Maternity Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
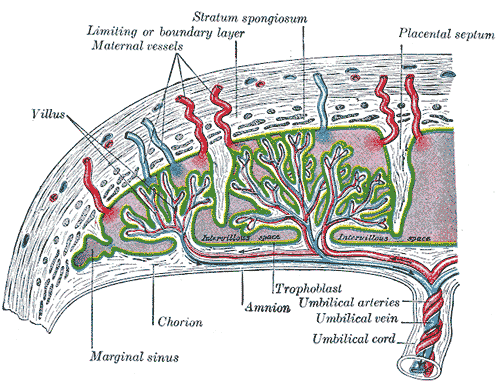
Consider the physiological engineering required to build and sustain a new human being. The maternal body must radically alter its own hemodynamic, endocrine, and structural baselines to construct a temporary, high-flow life-support system—the placenta—while simultaneously accommodating a rapidly growing passenger. For a nurse operating on a busy maternity ward in Riyadh or Jeddah, anticipating the failure points of this system is not merely academic; it is the difference between a routine delivery and an avoidable catastrophe. Maternity nursing is applied physics, fluid dynamics, and pharmacology intersecting at the bedside. To master the Saudi Nursing Licensure Examination (SNLE), one must stop memorizing disconnected obstetrical facts and start understanding the mechanical and biochemical why behind maternal-fetal adaptations.
When a woman presents to the antenatal clinic, the first objective is to quantify her obstetrical history. We do this not with a narrative, but with precise numerical coordinates.
Gravidity refers to the total number of times a woman has been pregnant, regardless of the outcome. Parity is the number of pregnancies that have reached 20 weeks of gestation, regardless of whether the fetus was born alive. To provide greater clinical resolution, we rely on the GTPAL system, which parses her history into Gravidity, Term births, Preterm births, Abortions, and Living children.
Diagnostics and Dating
To predict the operational timeline of the pregnancy, we calculate the estimated date of delivery using Naegele's rule: subtract three months and add seven days to the first day of the last menstrual period.
But is she actually pregnant? We divide the signs of pregnancy into three categories based on diagnostic certainty:
- Probable signs: A positive pregnancy test detecting human chorionic gonadotropin (hCG) is classified as a probable sign of pregnancy. It strongly suggests pregnancy, but hydatidiform moles or certain tumors can also secrete hCG.
- Positive signs: Absolute confirmation requires direct evidence of the fetus. Fetal heart tones auscultated by a Doppler device constitute a positive sign of pregnancy.
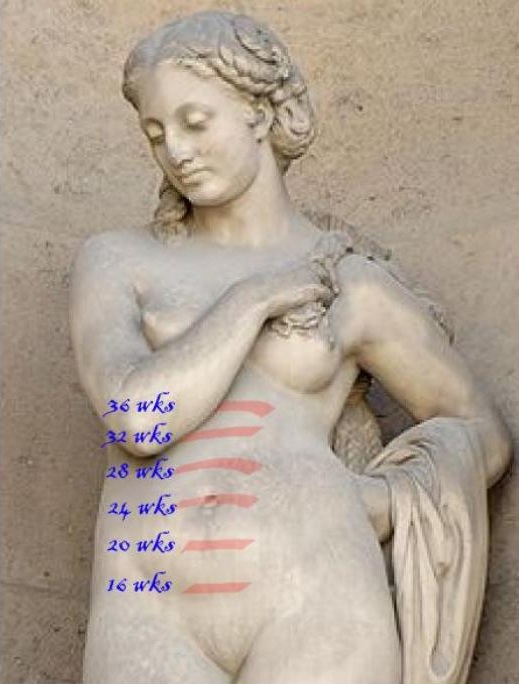
Once confirmed, we monitor fetal growth mechanically. Between 18 and 32 weeks of gestation, the fundal height in centimeters approximately equals the fetal age in weeks. If a mother is 24 weeks pregnant, her fundus should measure roughly 24 centimeters from the pubic symphysis.
Maternal System Upgrades and Adaptations
To perfuse two organisms, the maternal cardiovascular system must expand. Maternal cardiac output increases by 30 to 50 percent during a normal pregnancy.
However, this increased fluid volume runs through a compromised plumbing system. The inferior vena cava (IVC) is a low-pressure return pipe running slightly to the right of the maternal spine. When a pregnant woman lies flat on her back, the heavy, fluid-filled gravid uterus compresses this pipe. This causes supine hypotensive syndrome, drastically reducing venous return and dropping maternal blood pressure. The physics dictate the solution: placing a wedge under the pregnant woman's right hip prevents supine hypotensive syndrome by tilting the uterus to the left, physically lifting it off the IVC.
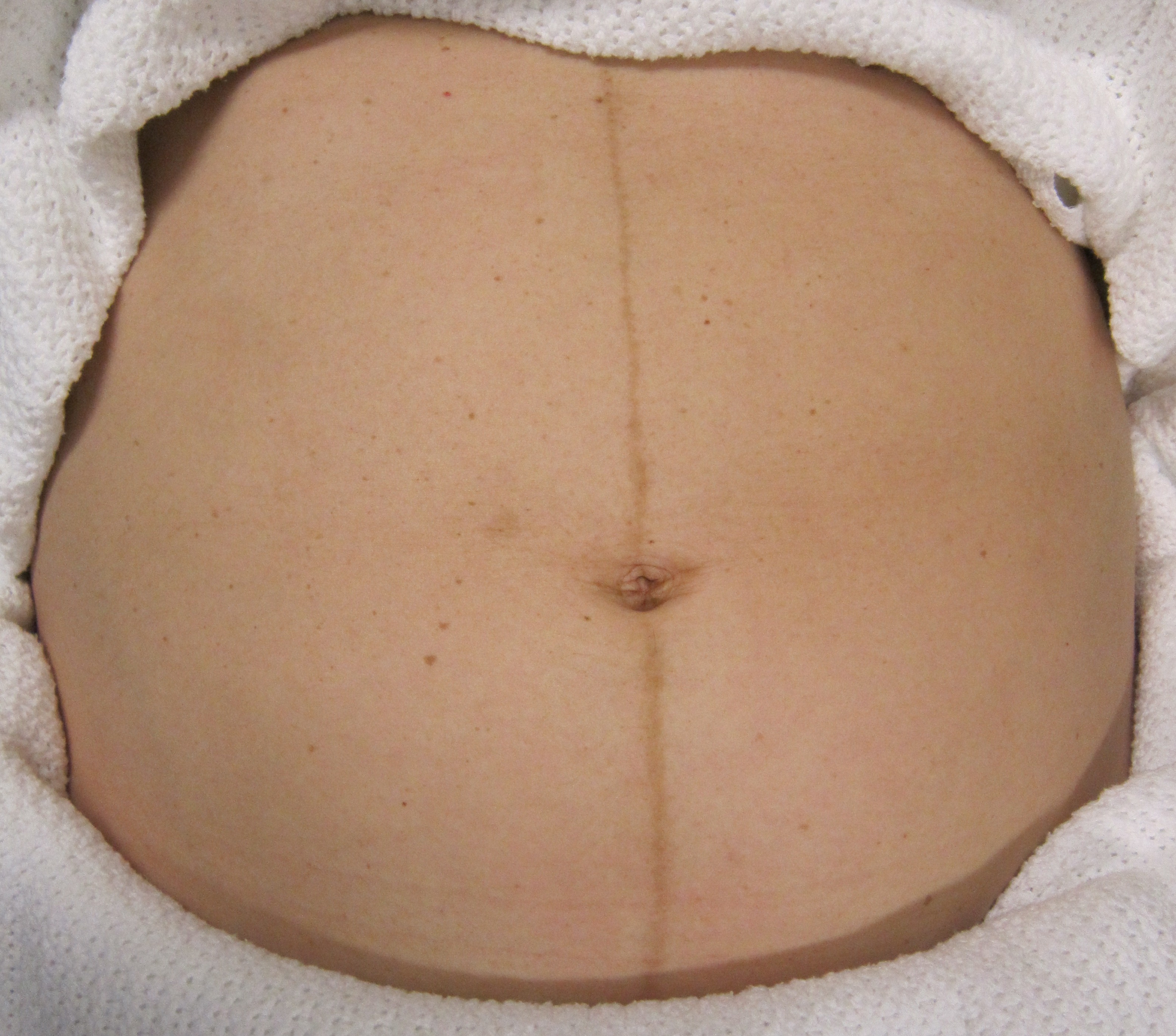
Pregnancy also shifts maternal biochemistry. The endocrine cascade causes dermatological changes, including chloasma (a brownish hyperpigmentation of the facial skin, often called the "mask of pregnancy") and the linea nigra (a pigmented line extending from the symphysis pubis to the top of the fundus).
Neurologically, the mother will first feel the fetus move—a phenomenon known as quickening, which is the maternal perception of fetal movement. Quickening typically occurs between 16 and 20 weeks of gestation.
Antenatal Requirements
To support this rapid cell division and prevent structural errors in the fetus, folic acid supplementation of 400 micrograms daily is recommended before and during early pregnancy to prevent neural tube defects.
Because of the increased blood volume, breast tissue, placenta, and fetus, the normal weight gain during pregnancy for a woman with a normal body mass index is 25 to 35 pounds.
Pregnancy operates at the absolute physiological limit. When the system is pushed past this limit, life-threatening complications emerge.
Hemorrhagic and Implantation Errors
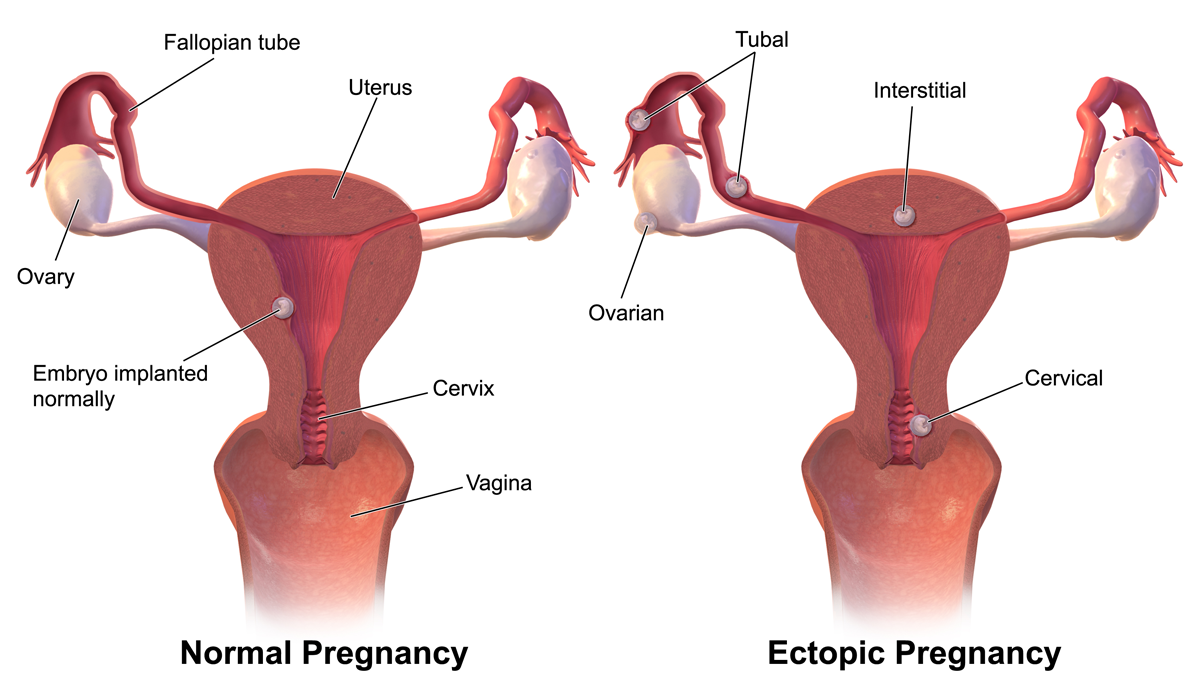
If an embryo implants outside the endometrial cavity, the surrounding tissues cannot stretch to accommodate it. An ectopic pregnancy most commonly occurs in the ampulla of the fallopian tube. If this tube bursts, a ruptured ectopic pregnancy typically presents with unilateral abdominal pain and referred shoulder pain (caused by blood pooling under the diaphragm and irritating the phrenic nerve).
Later in pregnancy, bleeding usually originates from the placenta. You must distinguish between two primary placental crises based on a simple clinical picture:
- Placenta Previa: The placenta implants over the cervical os. As the cervix softens, vessels tear. Placenta previa presents with painless bright red vaginal bleeding during the second or third trimester. Because the placenta is blocking the exit, vaginal examinations are strictly contraindicated in cases of suspected placenta previa—a blind finger could puncture the placenta and cause catastrophic hemorrhage.
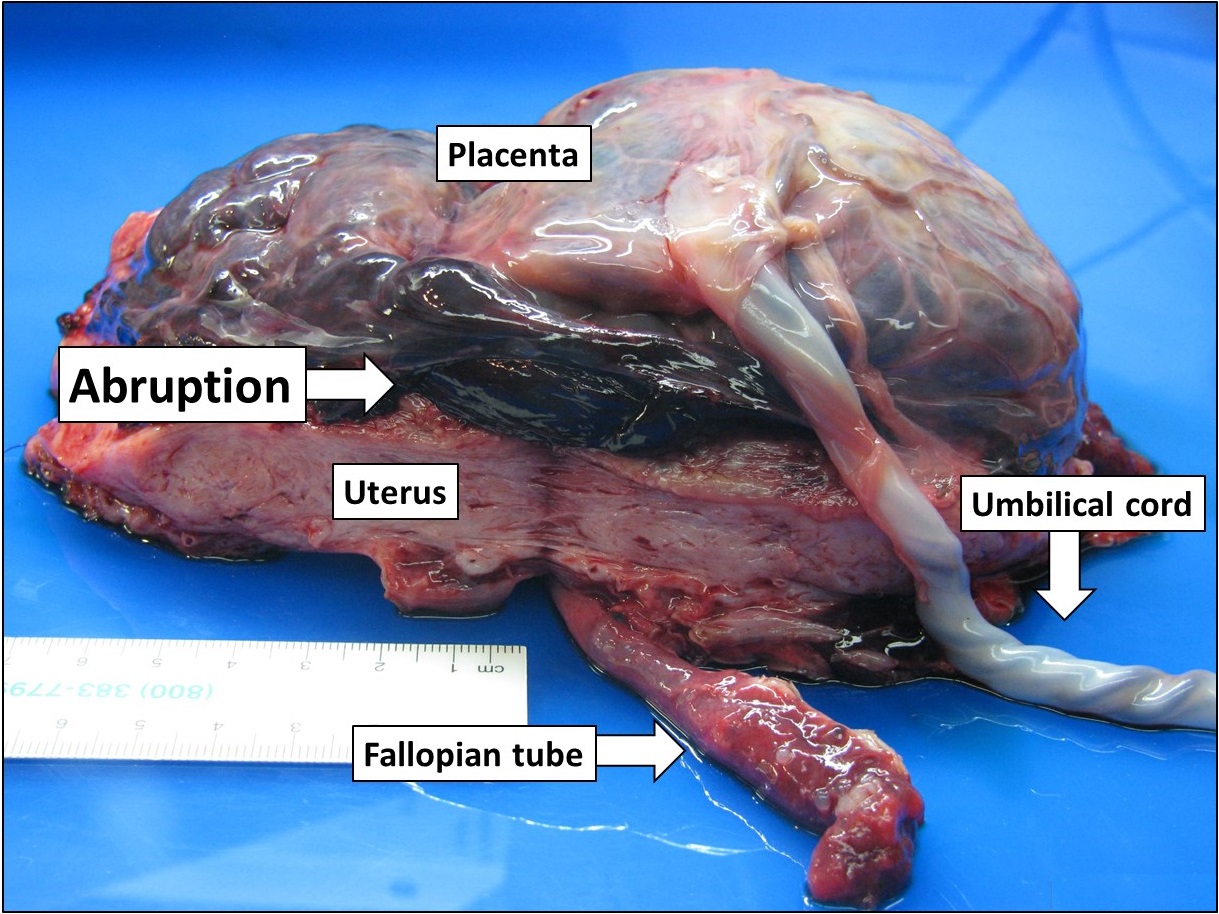
- Abruptio Placentae: The placenta prematurely rips away from the uterine wall. Because blood is trapped behind the placenta, tearing the highly innervated uterine muscle, abruptio placentae is characterized by sudden onset of severe abdominal pain and dark red vaginal bleeding.
Hypertensive Disorders
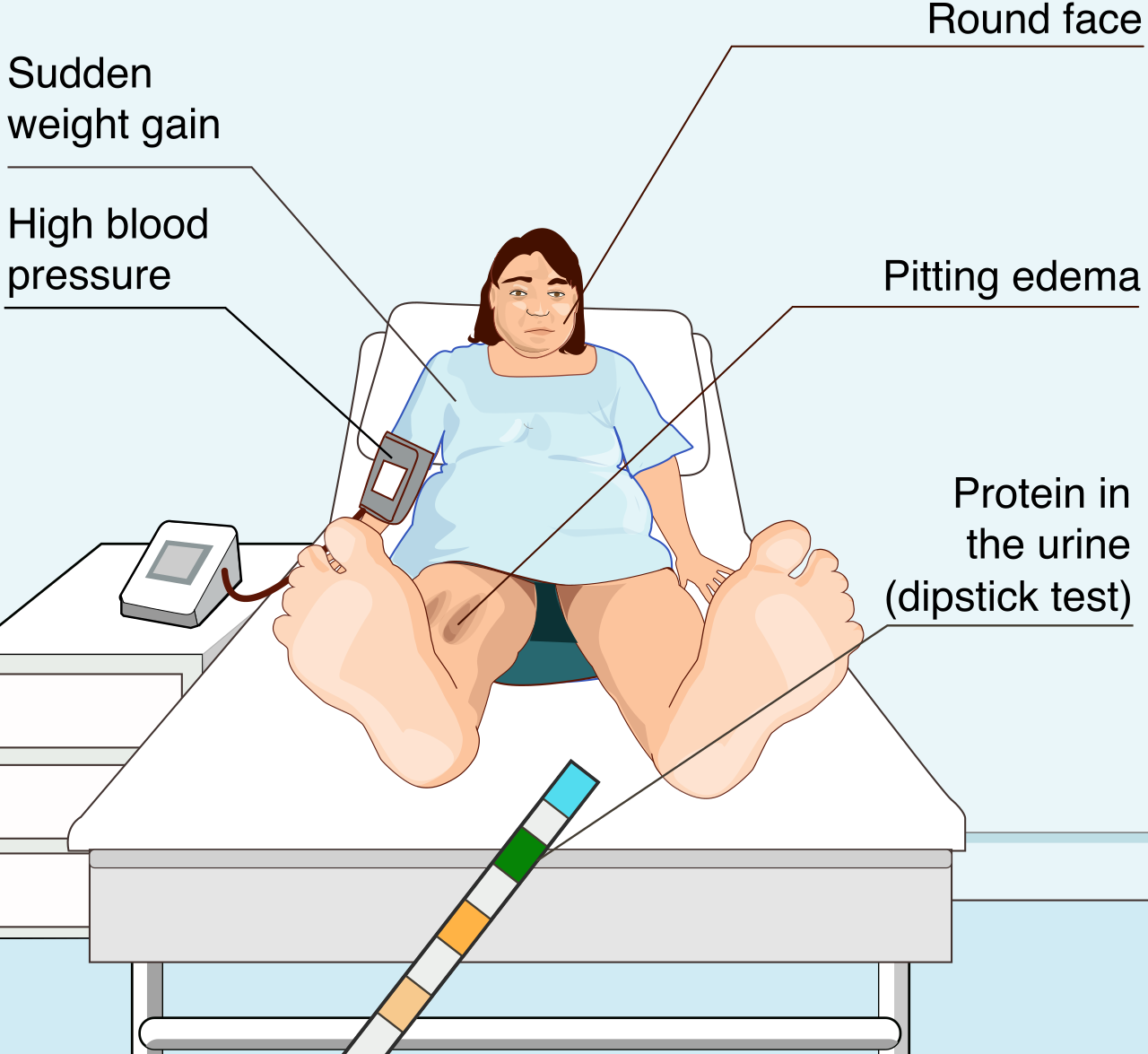
Preeclampsia is a disorder of pregnancy characterized by new-onset hypertension and proteinuria after 20 weeks of gestation. It is a disease of widespread endothelial dysfunction. Vasospasm damages the kidneys (proteinuria) and the brain (hyperreflexia and seizures).
To prevent the brain from seizing, we administer a central nervous system depressant. Magnesium sulfate is administered to patients with severe preeclampsia to prevent seizures. However, magnesium is a dangerous drug; it essentially turns down the volume on the entire nervous system. The therapeutic range for serum magnesium levels during magnesium sulfate therapy is 4 to 7 mEq/L.
If the level creeps too high, the nervous system shuts down completely. Therefore, loss of deep tendon reflexes is an early clinical sign of magnesium sulfate toxicity. If toxicity occurs, you must immediately reverse the blockade: calcium gluconate is the pharmacological antidote for magnesium sulfate toxicity.
If preeclampsia goes unchecked, it can degrade into HELLP syndrome, which stands for Hemolysis, Elevated Liver enzymes, and Low Platelets. This is a multisystem failure requiring immediate delivery.
Metabolic and Immunologic Clashes
Pregnancy is inherently diabetogenic because placental hormones create insulin resistance to ensure plenty of glucose remains in the blood for the fetus. If the mother's pancreas cannot overcome this resistance, she develops Gestational Diabetes Mellitus. We screen for this because gestational diabetes mellitus increases the risk of fetal macrosomia (a large fetus), complicating delivery. A one-hour oral glucose tolerance test is typically performed between 24 and 28 weeks of gestation.
We must also prevent the maternal immune system from attacking the fetus. If a mother has Rh-negative blood and her fetus is Rh-positive, her body may produce antibodies against the fetal blood. To hide the fetal antigens from the mother's immune system, Rho(D) immune globulin is administered at 28 weeks of gestation to all Rh-negative pregnant women. Furthermore, Rho(D) immune globulin must be administered within 72 hours after birth if an Rh-negative mother delivers an Rh-positive infant.
Gastrointestinal and Fluid Imbalances
While mild nausea is normal, hyperemesis gravidarum is severe nausea and vomiting during pregnancy leading to weight loss and dehydration. Because the mother is starving, her body begins breaking down fat for energy. Consequently, ketonuria is a common laboratory finding in clients with hyperemesis gravidarum.
The amniotic fluid surrounding the fetus serves as a cushion and allows for musculoskeletal development. Deviations in fluid volume indicate underlying pathology:
- Oligohydramnios is defined as an abnormally low volume of amniotic fluid, often indicating fetal renal agenesis or poor placental perfusion.
- Polyhydramnios is an excess of fluid. Because the uterus is a muscle, stretching it too far reduces its ability to snap back after birth. Therefore, polyhydramnios increases the risk of postpartum hemorrhage due to uterine overdistension.
Maternal Infection and Coagulation Risks
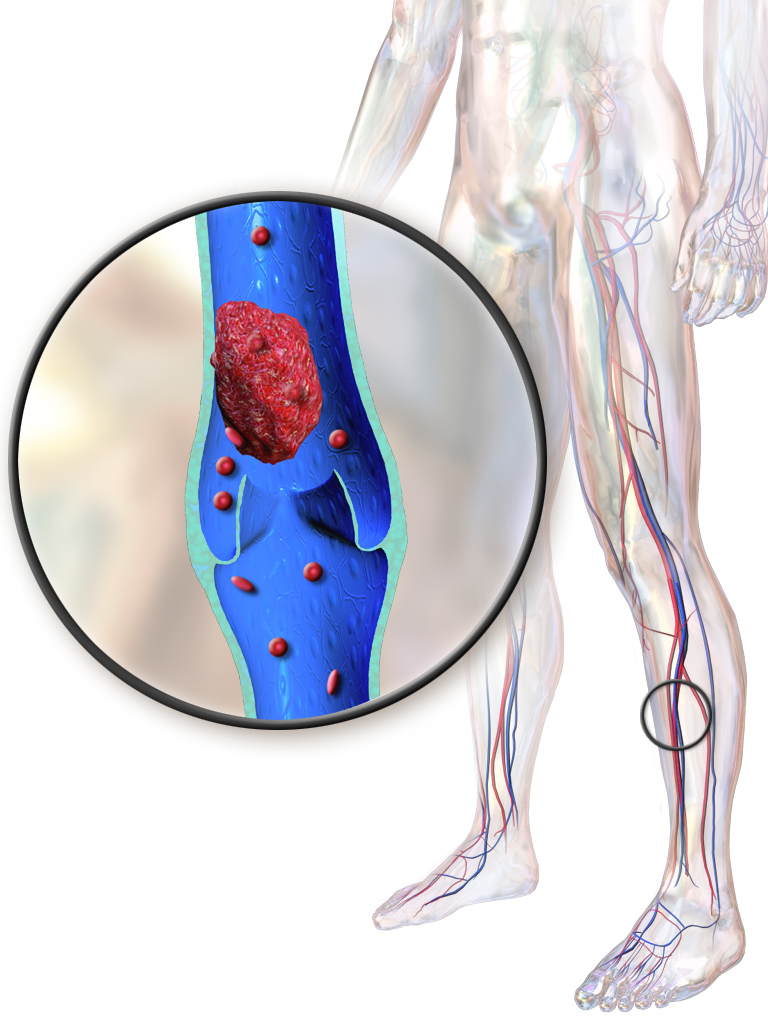
Pregnancy is a hypercoagulable state. The body ramps up clotting factors to prepare for the massive vascular severance that occurs when the placenta detaches. The trade-off is that pregnant women have an increased physiological risk of developing deep vein thrombosis.
Dietary and viral exposures also pose severe risks:
- Pregnant women should avoid consuming unpasteurized dairy products to prevent Listeria infection, which can cause miscarriage or stillbirth.
- Maternal rubella infection during the first trimester can cause congenital cataracts and deafness in the fetus. However, the rubella vaccine is contraindicated during pregnancy due to its live-attenuated nature. It must be given postpartum.
Labor is the mechanical process of opening the cervical door and pushing the passenger through the pelvic bony cage.
Cervical Mechanics
To differentiate true labor from false alarms, look at the cervix. True labor contractions cause progressive cervical dilation and effacement. In contrast, false labor contractions do not result in progressive cervical change.
- Effacement is the shortening and thinning of the cervix during labor.
- Dilation is the widening of the cervical opening during labor.
The Stages of Labor
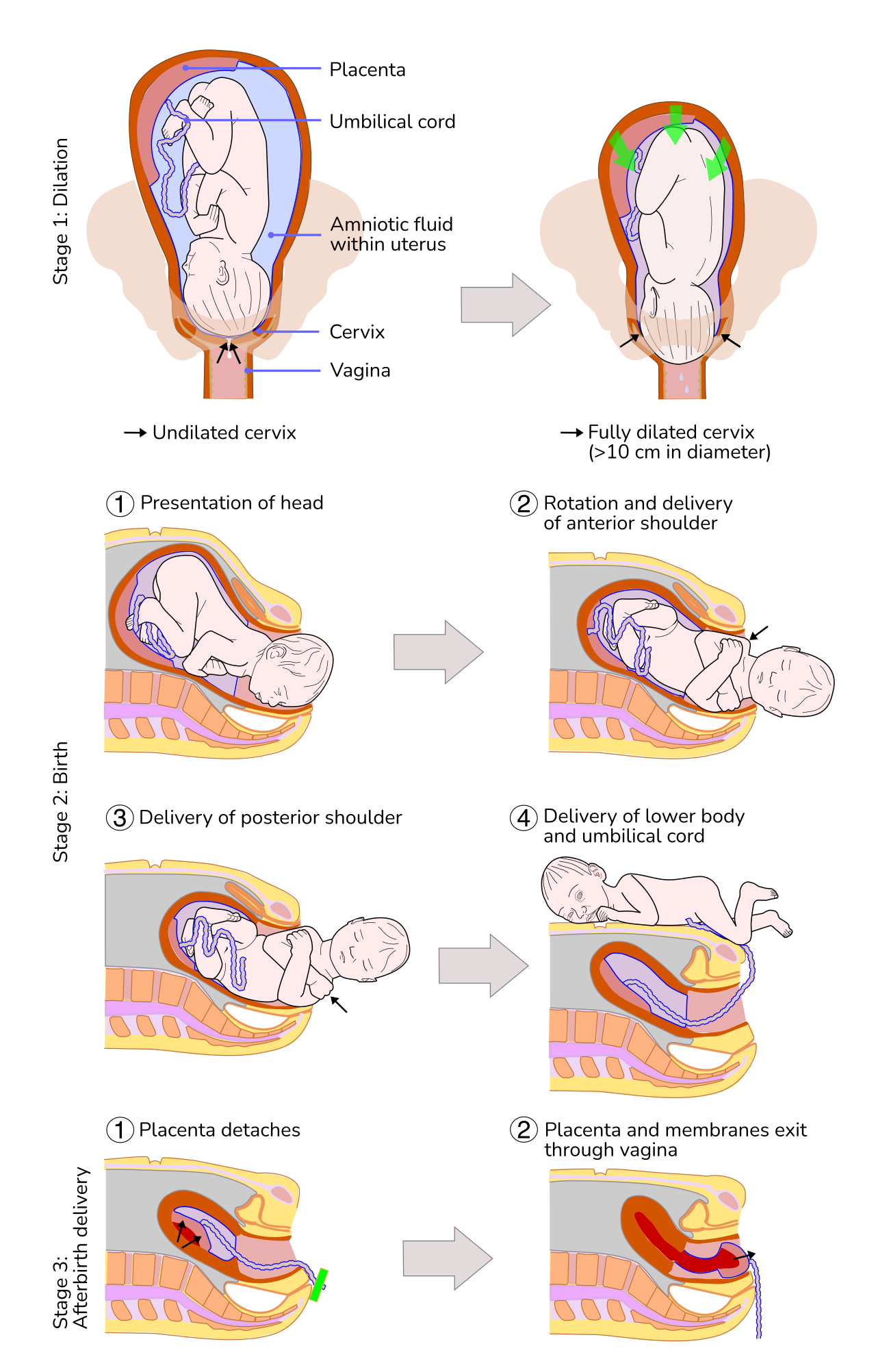
Labor is mathematically divided into four distinct stages:
The first stage of labor involves cervical dilation from 0 to 10 centimeters. It is subdivided into three phases:
- The latent phase of the first stage of labor is characterized by cervical dilation of 0 to 3 centimeters.
- The active phase of the first stage of labor involves cervical dilation of 4 to 7 centimeters.
- The transition phase of the first stage of labor is marked by cervical dilation of 8 to 10 centimeters.
The second stage of labor spans from full cervical dilation to the birth of the neonate. This is the pushing stage. The third stage of labor begins after the birth of the neonate and ends with the delivery of the placenta. The fourth stage of labor represents the first one to four hours postpartum, the critical window for hemodynamic stabilization.
Measuring Fetal Descent
As the fetus descends, we measure its progress against the maternal pelvic bones. The station of the fetal presenting part is measured relative to the maternal ischial spines. A fetal station of zero indicates that the presenting part is exactly at the level of the maternal ischial spines (engagement). Negative numbers mean the fetus is floating higher; positive numbers indicate the fetus is crowning.
Interventions in Labor
If labor stalls or must be induced, we assess the cervix. A Bishop score of 8 or higher indicates a favorable cervix for successful induction of labor.
We may also perform an amniotomy, which is the artificial rupture of the amniotic membranes to induce or augment labor. When the fluid gushes out, the umbilical cord can wash down with it. Therefore, the immediate nursing priority after an amniotomy is to assess the fetal heart rate to ensure the cord has not prolapsed.
To drive contractions, we use synthetic hormones. The hormone oxytocin stimulates uterine contractions during labor. For analgesia, an epidural anesthesia commonly causes maternal hypotension due to widespread sympathetic blockade and vasodilation. To counteract this physics problem, administering an intravenous fluid bolus before an epidural helps prevent maternal hypotension. Alternatively, a pudendal nerve block provides perineal anesthesia during the second stage of labor without affecting maternal blood pressure.
Fetal Heart Rate Interpretation
The fetus is entirely dependent on the placenta for oxygen during the crushing forces of uterine contractions. The normal baseline fetal heart rate ranges from 110 to 160 beats per minute.
To assess fetal well-being before labor, we use a nonstress test. A nonstress test is considered reactive if there are two fetal heart rate accelerations within a 20-minute period.
During labor, decelerations tell us exactly what the fetus is experiencing:
- Early decelerations in the fetal heart rate are caused by fetal head compression during uterine contractions. These mirror the contraction and are benign.
- Variable decelerations in the fetal heart rate indicate umbilical cord compression. They look like sharp "V"s on the monitor.
- Late decelerations in the fetal heart rate signify uteroplacental insufficiency. The placenta is failing, and the fetus is running out of oxygen at the peak of the contraction. This is an emergency. Nursing interventions for late decelerations include repositioning the mother to her left side to maximize cardiac output and placental perfusion.
Intrapartum Complications
If the mother develops a fever during labor, suspect infection inside the amniotic sac. Maternal fever during labor is the most reliable indicator of chorioamnionitis.
If the baby needs to be delivered preterm, the lungs will lack surfactant. In these cases, betamethasone is administered to pregnant women at risk of preterm delivery to accelerate fetal lung maturity.
Two catastrophic mechanical failures can occur during delivery:
- Umbilical Cord Prolapse: The cord falls below the fetal head, cutting off all oxygen. In the event of an umbilical cord prolapse the nurse should immediately elevate the fetal presenting part off the cord with a gloved hand. Additionally, the knee-chest position is recommended to relieve pressure on a prolapsed umbilical cord.
- Shoulder Dystocia: The fetal head delivers, but the anterior shoulder gets stuck behind the maternal pubic bone. To fix this geometry, McRoberts maneuver is utilized to resolve shoulder dystocia during delivery (hyperflexing the maternal legs to the abdomen to flatten the sacrum). Applying suprapubic pressure during shoulder dystocia helps dislodge the anterior fetal shoulder. Crucially, fundal pressure is strongly contraindicated during instances of shoulder dystocia—pushing from the top only wedges the shoulder deeper and can rupture the uterus.

Once the placenta detaches, the highly vascularized uterine wall is essentially an open wound. The only way the body can stop the bleeding is by clamping the muscle fibers tightly around the torn vessels.
Postpartum Hemorrhage
If the uterus fails to contract, the mother will bleed out. Uterine atony is the most common cause of postpartum hemorrhage.
Clinically, postpartum hemorrhage is defined as a blood loss greater than 500 milliliters after a vaginal delivery, and a blood loss greater than 1000 milliliters after a cesarean section.
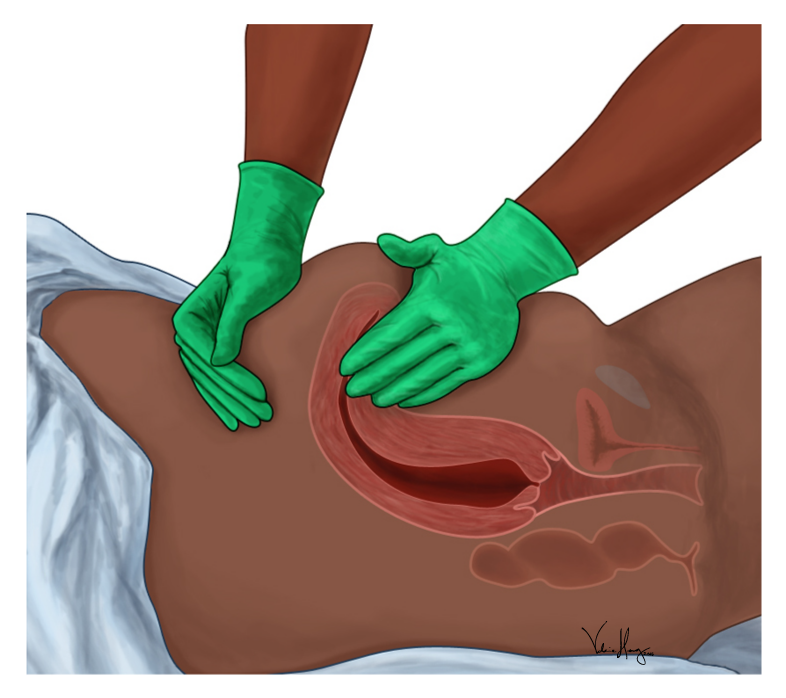
How do you know the uterus is failing? A boggy uterus indicates uterine atony. It feels like a soft sponge rather than a firm grapefruit. Fundal massage is the initial nursing intervention for a boggy postpartum uterus to manually stimulate muscular contraction.
Mechanically, the uterus sits right behind the bladder. A full bladder can displace the postpartum uterus and cause uterine atony. If the fundus is deviated to the right and above the umbilicus, catheterize the patient or assist her to void.
Postpartum Healing and Exudate
As the uterine lining heals, it sloughs off tissue and blood, known as lochia. The timeline of lochia acts as a biological clock for postpartum healing:
- Lochia rubra is a dark red vaginal discharge occurring in the first three to four days postpartum.
- Lochia serosa is a pinkish-brown vaginal discharge occurring from approximately day four to day ten postpartum.
- Lochia alba is a yellowish-white vaginal discharge occurring from approximately day eleven to six weeks postpartum.
Lactation and Breast Care
The endocrine shift after placental delivery initiates lactation. Prolactin is the anterior pituitary hormone responsible for maternal milk production. Once the milk is produced, oxytocin facilitates the milk let-down reflex during breastfeeding.
If the mother chooses not to breastfeed, her body will still produce milk, causing painful engorgement. Breast engorgement in non-breastfeeding mothers is managed with supportive bras and cold compresses. Furthermore, nipple stimulation should be avoided in non-breastfeeding postpartum mothers to prevent further milk production.
In breastfeeding mothers, blocked ducts can lead to infection. Mastitis is an infection of the breast tissue that typically presents with localized redness, warmth, and maternal fever. Because the infection is in the tissue (not the milk), mothers with mastitis should be encouraged to continue breastfeeding or pumping from the affected breast to clear the stasis.

Psychological Adaptation
The drastic hormonal crash postpartum alters neurochemistry. Most mothers experience mild emotional lability. Postpartum blues are transient mild depressive symptoms that typically resolve within two weeks after delivery. However, if these symptoms deepen and persist, it crosses the line into clinical pathology. Postpartum depression is characterized by pervasive sadness and lack of interest persisting beyond two weeks after delivery. Recognizing this distinction is a critical nursing responsibility on any postnatal ward, ensuring the mother remains safe to care for the infant she just spent nine months building.