Nursing Teams and Interprofessional Relations
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
In a high-acuity intensive care unit in Riyadh, the survival of a patient with multisystem organ failure does not depend solely on the solitary brilliance of a single physician or the isolated vigilance of a primary nurse. It depends on the invisible connective tissue between the professionals in the room. The respiratory therapist adjusting the ventilator, the clinical pharmacist calculating renal clearance, the attending physician diagnosing the underlying pathology, and the bedside nurse coordinating the moment-to-moment physiologic demands are not acting in a vacuum. They form a deeply interconnected network where communication failures are mathematically proven to result in patient harm. Understanding how to orchestrate this network—how to lead, how to communicate, and how to resolve the inevitable friction of clinical practice—is the foundation of modern nursing leadership.
The Saudi Nursing Licensure Examination (SNLE) tests not just your clinical knowledge, but your ability to operate safely and effectively within this complex human system.
Leadership is not merely a title; it is the deliberate application of influence to achieve specific outcomes. In the dynamic environment of a hospital ward, a single leadership style is insufficient. The most effective nurses adapt their approach to the situational demands of the patient and the team.
- Transformational leadership inspires followers to exceed expectations by appealing to higher ideals and shared values. These leaders do not just manage; they fundamentally elevate the clinical environment. Transformational leaders in nursing foster environments that promote evidence-based practice and continuous learning. When a charge nurse inspires her team to adopt a new, evidence-based pressure ulcer prevention protocol because it aligns with their core mission of healing, she is utilizing transformational leadership.
- Democratic leadership involves seeking input from team members before making operational decisions. By giving the staff a voice, democratic leadership increases staff motivation and commitment to shared community goals.
- Autocratic leadership relies on centralized decision-making with minimal input from subordinate staff. While this sounds oppressive for daily ward management, it is highly situational. Autocratic leadership is highly effective during emergency clinical situations requiring immediate direction. During a Code Blue, the team leader does not ask for a consensus on whether to administer epinephrine; they issue a direct, autocratic command.
- Servant leadership turns the traditional hierarchy upside down. It prioritizes the needs and growth of team members over the personal ambitions of the leader. The servant leader asks, "What barriers can I remove today so you can provide better care?"
- Transactional leadership operates on a simple exchange mechanism. It uses rewards and punishments to manage employee performance, such as offering preferred scheduling to nurses who pick up overtime shifts.
- Laissez-faire leadership involves a hands-off approach where team members make independent decisions. While it can work with highly specialized, self-motivated experts, in standard clinical settings, laissez-faire leadership frequently leads to role confusion and decreased productivity in unstructured nursing environments.
Leadership Beyond the Ward
Modern nursing extends beyond the walls of the acute care facility. Community-based nursing leadership focuses on health promotion and disease prevention within specific demographic populations. To achieve this, leaders utilize boundary spanning leadership, which connects internal nursing teams with external community resources to achieve broader population health goals.
Practicing in Saudi Arabia requires an understanding of the specific institutional and cultural frameworks guiding care. The Saudi Ministry of Health Vision 2030 healthcare transformation emphasizes interprofessional collaboration to improve population health outcomes. To realize this vision, there is a unified national competency framework that standardizes interprofessional collaboration expectations across all Saudi healthcare facilities.
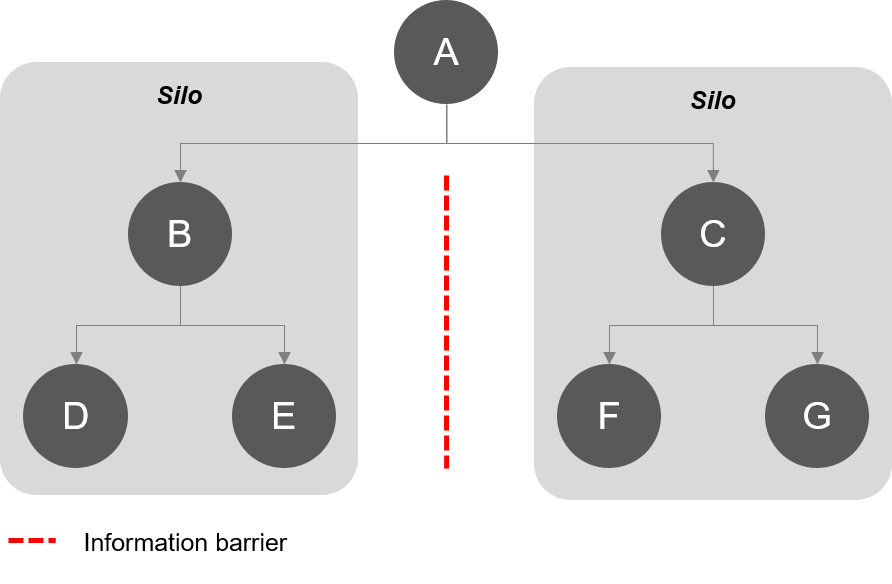
To ensure lifelong clinical competence, the Saudi Commission for Health Specialties (SCFHS) mandates continuing professional development (CPD) hours to maintain nursing licensure renewal. Furthermore, the SCFHS advocates for the integration of Interprofessional Education and Collaborative Practice. These Interprofessional Education and Collaborative Practice frameworks aim to break down academic silos in healthcare training, ensuring that nursing, medical, and pharmacy students learn to work together before they ever reach the clinical floor.
Culturally, practice in the Kingdom is distinct. Culturally competent leadership in Saudi Arabia requires integrating Islamic ethical principles into daily nursing management. Furthermore, culturally competent nursing leadership respects privacy and gender preferences prevalent in the Saudi healthcare context, ensuring that staffing and patient assignments honor these deeply held societal values.
We often use the words "team" loosely, but in healthcare organization, the structure dictates the function.
Multidisciplinary vs. Interdisciplinary
- A multidisciplinary team utilizes professionals from different disciplines who work independently with the same patient. Think of this like a relay race: the surgeon does her part, hands off to the ward nurse, who hands off to the physical therapist. Because of this parallel structure, multidisciplinary team members often communicate primarily through the medical record rather than direct consultation. However, an essential structural component of this model is that multidisciplinary rounds actively involve the patient and family in daily goal setting, ensuring the patient remains at the center of this fragmented expertise.
- An interdisciplinary team consists of professionals from various disciplines who communicate and collaborate to provide coordinated care. Think of this like a basketball team moving the ball together down the court. To maintain this coordination, interdisciplinary care conferences involve multiple healthcare disciplines meeting to align treatment plans.
Regardless of the model, true collaborative practice requires acknowledging the overlapping competencies of different healthcare professions. Furthermore, interprofessional collaboration involves sharing power and responsibilities among different healthcare disciplines. Why does this matter? Because data shows that joint decision-making between nurses and physicians reduces the incidence of hospital-acquired adverse events.
Empowering the Bedside Nurse
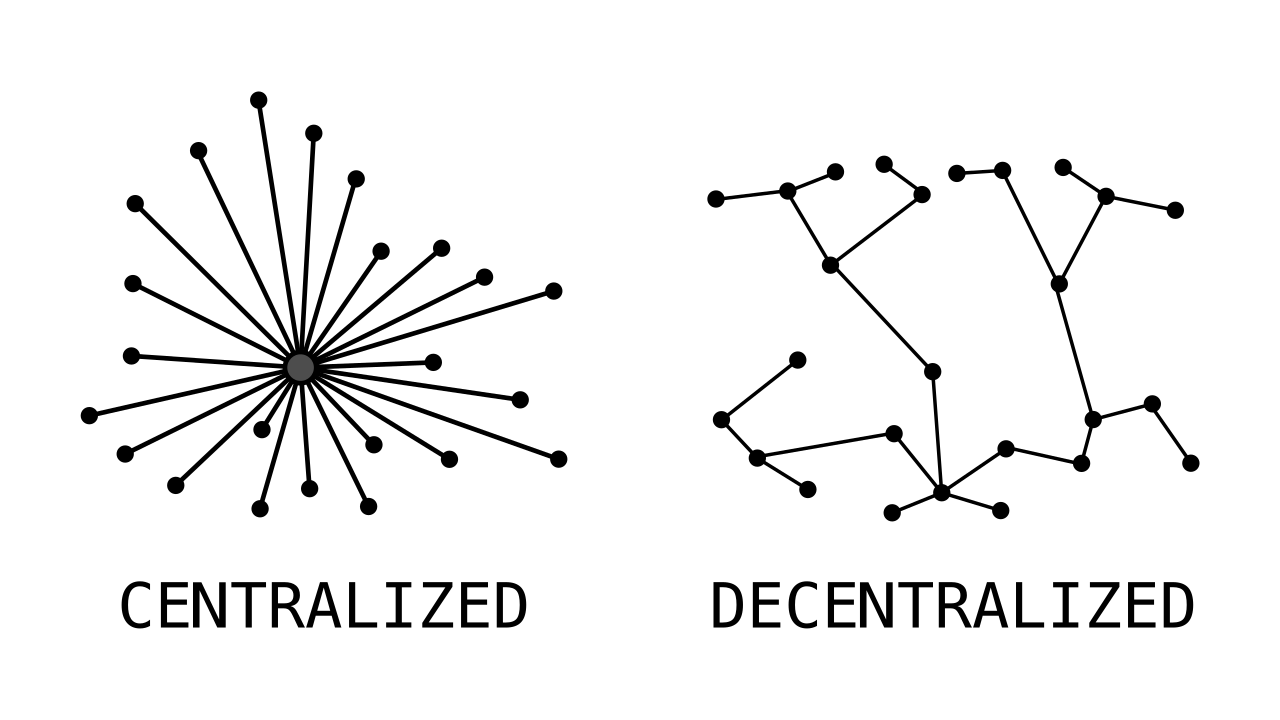
Healthcare institutions are moving away from top-down management toward shared governance, which is a nursing management model that decentralizes decision-making to empower clinical staff.
The Impact of Shared Governance: Giving nurses autonomy is not just an administrative courtesy; it is a clinical imperative. Empowering clinical bedside nurses in policy creation directly correlates with higher patient satisfaction scores. When the professionals delivering the care design the policies, the patient experience invariably improves.
All of these structures ultimately serve one goal: Patient-centered care, which prioritizes the individual values and preferences of the patient during clinical decision-making.
Communication is the central nervous system of a hospital. When it fails, patients suffer. The TeamSTEPPS program was developed by the Agency for Healthcare Research and Quality (AHRQ) to improve teamwork in healthcare settings. The entire TeamSTEPPS framework is designed to optimize healthcare team performance and improve patient safety through specific, highly structured communication tools.
Structured Communication Tools
- SBAR: SBAR stands for Situation, Background, Assessment, and Recommendation. SBAR provides a standardized framework to communicate critical patient information between healthcare professionals. By formatting a midnight call to a physician via SBAR, the nurse eliminates cognitive friction and delivers precisely what is needed to make a clinical decision.
- CUS: When immediate danger is present, politeness must give way to clarity. The CUS communication tool uses the phrases: I am Concerned, I am Uncomfortable, and This is a Safety issue. The CUS tool is utilized to respectfully halt patient care activities when a team member perceives an immediate risk.
- The Two-Challenge Rule: This rule empowers team members to stop clinical action if a safety concern is ignored after two verbal warnings. If you tell a physician they are about to break the sterile field, and they ignore you, you challenge them a second time. If ignored again, you have the institutional authority to halt the procedure.
Team Dynamics and Error Reduction
To prevent errors before they occur, high-functioning teams rely on cross-monitoring, which is an error reduction strategy where team members continuously monitor the actions of their colleagues. This is not micro-management; it is a safety net. This net is strengthened by mutual support, which involves anticipating the needs of other team members and providing assistance during high workload periods.
A well-orchestrated shift requires temporal markers. Regular interprofessional team briefings reduce clinical misunderstandings before shift commencement, setting the operational tempo. Conversely, debriefing sessions allow healthcare teams to reflect on critical incidents to improve future performance.
If a nurse identifies a systemic safety failure, they must know how to navigate the bureaucracy to fix it. Clear chain-of-command structures help nurses navigate bureaucratic hurdles when escalating patient safety concerns.
Where there is high stress, high stakes, and overlapping responsibilities, conflict is inevitable. In fact, role ambiguity among team members is a primary catalyst for interprofessional conflict. When it is unclear whether the nurse or the respiratory therapist is responsible for weaning a patient’s oxygen, friction occurs.
Conflict Resolution Styles
When managing disputes, professionals utilize different styles based on the stakes and the relationship:
| Style | Definition | Clinical Application |
|---|---|---|
| Collaborating | A conflict resolution style aiming for a win-win outcome by addressing the needs of all parties. | The ideal approach for complex care planning where all disciplines must agree on a cohesive path forward. |
| Compromising | Involves both parties giving up something of value to resolve a conflict. | Useful when time is limited and a temporary, mutually acceptable solution is required. |
| Accommodating | A conflict style where one party sacrifices their own needs to satisfy the other party. | Used when preserving the relationship is more important than the specific issue at hand. |
| Competing | An assertive and uncooperative conflict resolution style focused on a win-lose outcome. | Necessary when an unpopular but critical safety decision must be enforced immediately. |
| Avoiding | A conflict resolution style characterized by ignoring or withdrawing from the disagreement. | Only appropriate for trivial issues or when emotions are too high to achieve a rational resolution. |
The Role of Emotional Intelligence
Resolving these conflicts requires profound self-regulation. Emotional intelligence enables nurses to recognize and manage their own emotions during stressful clinical situations. By mastering their internal state, emotional intelligence enhances empathy and mutual respect when interacting with diverse healthcare colleagues.
During conflicts, humans communicate on multiple channels. Active listening requires the nurse leader to fully concentrate on the speaker rather than passively hearing the message. Furthermore, leaders must pay attention to what is not being said, as nonverbal communication often conveys more emotional truth than spoken words during interprofessional conflicts. When managing performance, constructive feedback must focus on objective behaviors rather than personal attributes. You critique the failure to document a vital sign, not the nurse's inherent work ethic.
Psychological Safety and Lateral Violence
None of these tools work in a toxic environment. Effective teams require psychological safety, which is the shared belief that a team environment is safe for interpersonal risk-taking. Why is this vital? Because high psychological safety encourages nurses to report near-misses without fear of punitive action. If a nurse fears being fired for an honest medication near-miss, they will hide it, and the systemic flaw will eventually kill a patient.
Conversely, environments lacking safety often breed lateral violence, which refers to hostile or aggressive behavior directed toward co-workers at the same organizational level. To combat this, healthcare institutions utilize zero-tolerance policies to eliminate workplace bullying and lateral violence.
A charge nurse cannot physically complete every task on the unit. Task prioritization by nurse managers ensures equitable distribution of workload among nursing teams. To manage this workload, leaders rely on the critical skill of delegation.
The Core Tenet of Delegation: Effective delegation requires the nurse leader to transfer responsibility for a task while retaining overall accountability. If you delegate a blood glucose check to a technician, the technician is responsible for doing it, but you are accountable for the patient's resulting glycemic control.
To ensure safety, delegation must strictly follow The Five Rights of Delegation, which include right task, right circumstance, right person, right direction, and right supervision. By utilizing these rights effectively, assigning appropriate tasks to unlicensed assistive personnel (UAP) frees registered nurses to focus on complex patient assessments.
Finally, as healthcare continuously evolves, nurses are frequently called upon to implement new protocols. Effective change management requires identifying key stakeholders to build commitment for new clinical initiatives. To ensure everyone is pulling in the same direction during these transitions, a shared vision statement aligns the daily efforts of interdisciplinary team members toward common organizational goals.
Understanding these concepts is not merely an academic exercise for passing the SNLE; it is the blueprint for thriving as a professional nurse. By mastering the dynamics of the interprofessional team, you safeguard your patients, elevate your colleagues, and meaningfully contribute to the transformation of healthcare in Saudi Arabia.