Research and Evidence Based Practice
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
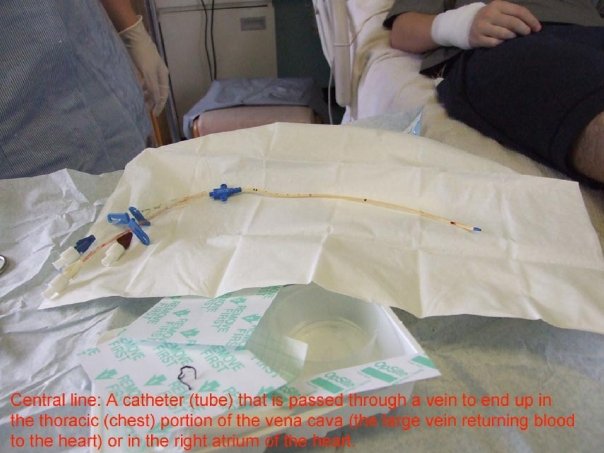
Consider the routine application of a chlorhexidine dressing for a central venous catheter in a bustling intensive care unit in Riyadh. The decision to use this specific protocol did not emerge from habit or guesswork; it is the culmination of decades of rigorous testing, statistical validation, and clinical observation. Every action you take at the bedside—from how you position a patient to prevent ventilator-associated pneumonia, to the methods you use to manage postoperative pain—relies on a foundation of scientific inquiry.
Nursing is not merely the execution of tasks; it is an applied science. For the Saudi Nursing Licensure Examination (SNLE), mastering the concepts of research and evidence-based practice is not just about passing a test. It is about understanding the very architecture of clinical excellence. You must know how to ask the right questions, how to evaluate the evidence you find, and how to safely and ethically translate that evidence into care that respects the cultural and individual nuances of your patients.
At its core, evidence-based practice integrates the best available research evidence with clinical expertise and patient values. This is a triad; if any one pillar is missing, the practice is incomplete.
- Clinical expertise refers to the proficiency and clinical judgment acquired through nursing experience. An expert nurse intuitively recognizes the subtle deterioration of a septic patient before the monitor alarms sound.
- Patient values encompass the unique preferences and expectations each patient brings to a clinical encounter. Integrating patient preferences into evidence-based practice requires the nurse to explain research findings in culturally appropriate language. If a family in Jeddah prefers to exhaust all palliative measures at home rather than in the hospital, the nurse must synthesize the evidence regarding home care with those deeply held cultural and personal values.
To execute EBP, nurses follow a rigorous, step-by-step methodology:
- Step 0: Step zero of the evidence-based practice process involves cultivating a spirit of inquiry within the healthcare environment. Before you can answer a question, you must be curious enough to ask it. Why do we perform Foley catheter care this way? Is there a better method?
- Step 1: The first step of the evidence-based practice process is asking the clinical question in a specific standardized format.
- Step 2: The second step of the evidence-based practice process is searching for the most relevant research evidence.
- Step 3: The third step of the evidence-based practice process is critically appraising the gathered evidence for validity and reliability.
- Step 4: The fourth step of the evidence-based practice process involves integrating the research evidence with clinical expertise and patient preferences. Clinical decision-making requires nurses to synthesize best research evidence with immediate patient assessment data.
- Step 5: The fifth step of the evidence-based practice process is evaluating the clinical outcomes of the practice decision. Did the new protocol actually reduce infection rates on your ward?
- Step 6: The sixth step of the evidence-based practice process is disseminating the outcomes of the clinical decision to stakeholders. You share your findings through huddles, presentations, or publications so other wards can benefit.
Formulating the Question: The PICOT Framework
You cannot search a medical database effectively by typing "How do I stop bedsores?" You must speak the language of clinical research. The PICOT framework is a standard method used by nurses to formulate searchable clinical questions.
| Letter | Component | Definition | SNLE Clinical Example |
|---|---|---|---|
| P | Population | The Patient population of interest. | Adult intensive care patients |
| I | Intervention | The Intervention or area of interest. | Application of prophylactic sacral foam dressings |
| C | Comparison | The Comparison intervention or comparison group. | Standard barrier cream protocol |
| O | Outcome | The Outcome of interest. | Reduction in hospital-acquired pressure injuries |
| T | Time | The Time required for the intervention to achieve a specific outcome. | Over a two-week admission period |
Not all evidence is created equal. A passing remark by a senior physician does not carry the same weight as a global statistical analysis of ten thousand patients. The hierarchy of evidence ranks research study designs based on the strength and reliability of the evidence provided. Imagine a pyramid: the peak represents the most robust, least biased evidence, while the base relies on observation and opinion.
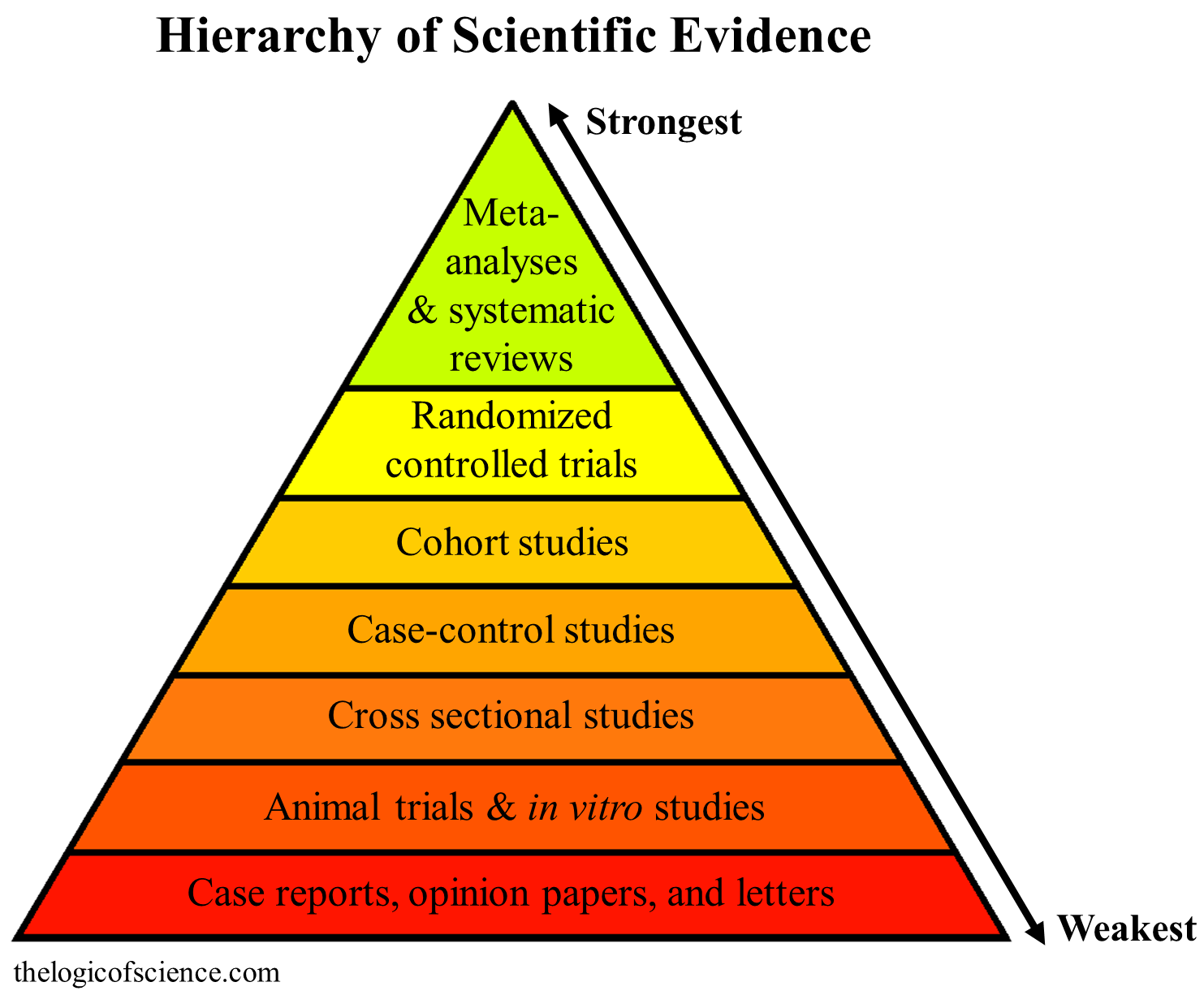
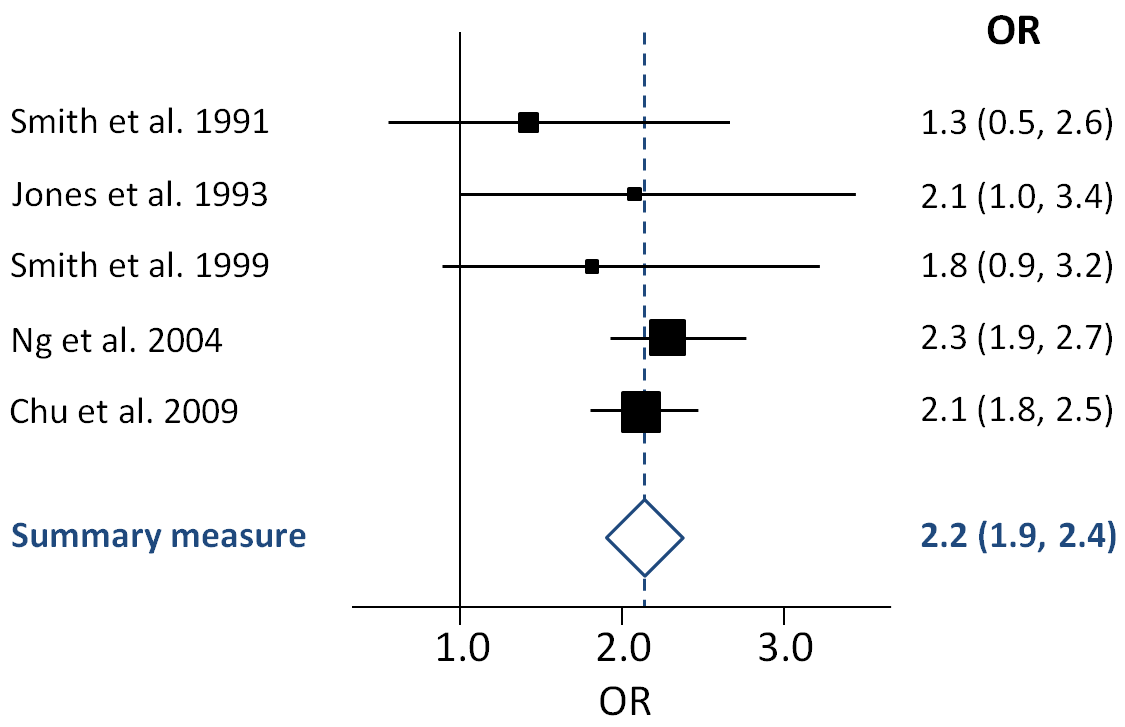
- Level I: This is the gold standard. Level I evidence consists of systematic reviews and meta-analyses of randomized controlled trials. Why is this so powerful? Because a meta-analysis statistically combines the results of multiple independent studies to produce a single estimate of an intervention effect. It removes the statistical "noise" of a single small study.
- Level II: Level II evidence is derived from at least one well-designed randomized controlled trial.
- Level III: Level III evidence comes from well-designed controlled trials without randomization. (Also known as quasi-experimental designs).
- Level IV: Level IV evidence originates from well-designed case-control studies and cohort studies.
- Level V: Level V evidence comes from systematic reviews of descriptive and qualitative studies.
- Level VI: Level VI evidence is derived from a single descriptive or qualitative study.
- Level VII: Level VII evidence is based on the opinion of authorities or reports from expert committees.
Exam Tip: When an SNLE question asks for the "highest level of evidence" to guide a clinical protocol, always look for systematic reviews or meta-analyses first. If those are absent, look for a randomized controlled trial (RCT).
Nursing research generates new knowledge intended for generalization to other populations and healthcare settings. This is distinct from internal problem-solving. Research is broadly categorized into quantitative (numbers) and qualitative (meaning).
Quantitative Research
Quantitative research focuses on numerical data and statistical analysis to test scientific hypotheses. It seeks objective, measurable truth.
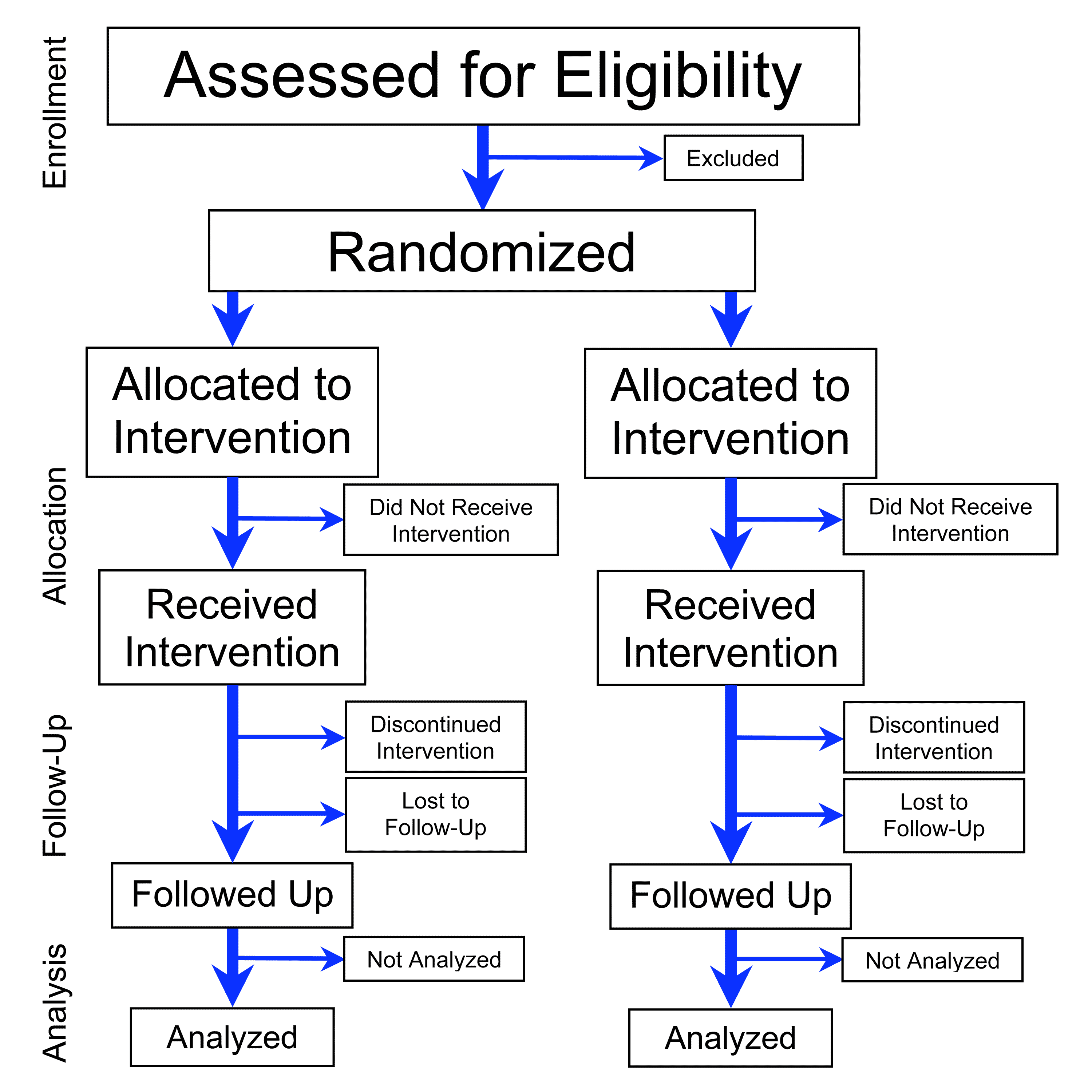
- Randomized Controlled Trial (RCT): A study that randomly assigns participants into an experimental group and a control group to measure the effect of an intervention. Randomization is the magic bullet that eliminates selection bias.
- Quasi-experimental research: Sometimes, random assignment is unethical or impossible. This design evaluates the effect of an intervention without using random assignment of participants.
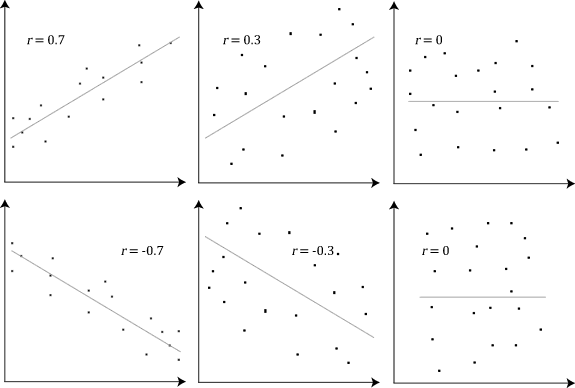
- Correlational research: This examines the statistical relationship between two or more variables without establishing cause and effect. (e.g., Observing that high nurse-to-patient ratios correlate with increased medication errors, though you cannot mathematically prove one caused the other without an experiment).
- Descriptive research: A design that observes and documents the characteristics of a population without manipulating any variables.
In quantitative studies, you must identify the levers the researcher is pulling and the dials they are reading:
- Independent variables are the specific interventions manipulated by the researcher during a study. (e.g., The type of IV dressing applied).
- Dependent variables are the specific outcomes measured by the researcher during a study. (e.g., The rate of phlebitis). The dependent variable depends on what you did.
Qualitative Research
Not everything important in nursing can be counted. Qualitative research explores the meaning of human experiences through non-numerical data like interviews and observations.
- Phenomenological research: This approach investigates the lived experiences of individuals regarding a specific life event. (e.g., Interviewing breast cancer survivors in Riyadh about their experience undergoing chemotherapy).
- Ethnographic research: Originating in anthropology, this involves immersing the researcher in a specific culture to understand the social dynamics of that group. (e.g., A researcher spending six months in a rural Saudi primary care clinic to understand the cultural dynamics of tribal health-seeking behaviors).
- Grounded theory research: Rather than starting with a hypothesis, this design aims to develop a theoretical framework derived inductively from collected interview data. The Grounded theory is "grounded" in the raw data itself.
Selecting the Participants: Sampling Methods
Researchers rarely study an entire population; they select a sample.
- Random sampling ensures every individual in the target population has an equal chance of being selected for the research study. This allows findings to be generalized.
- Convenience sample: A sample that consists of participants who are readily available and easily accessible to the researcher. (e.g., Surveying the nurses who happen to be working on your shift).
- Purposive sampling: A non-probability method where researchers intentionally select participants based on specific required characteristics. (e.g., If you are studying the lived experience of neonatal demise, you purposely seek out parents who have endured this specific tragedy).
Before launching a massive study, researchers often conduct a pilot study, which is a small-scale preliminary investigation conducted to evaluate feasibility and improve the study design before the main research begins. Think of it as a dress rehearsal.
If you weigh a patient three times on the same scale, and it reads 70 kg, 85 kg, and 62 kg, the scale is useless. Reliability refers to the consistency and repeatability of the measurement tool used in a research study.
However, if the scale reads exactly 90 kg three times in a row, but the patient actually weighs 75 kg, the scale is reliable, but invalid. Validity indicates the degree to which a research instrument accurately measures the intended concept.
We look at two dimensions of validity in research design:
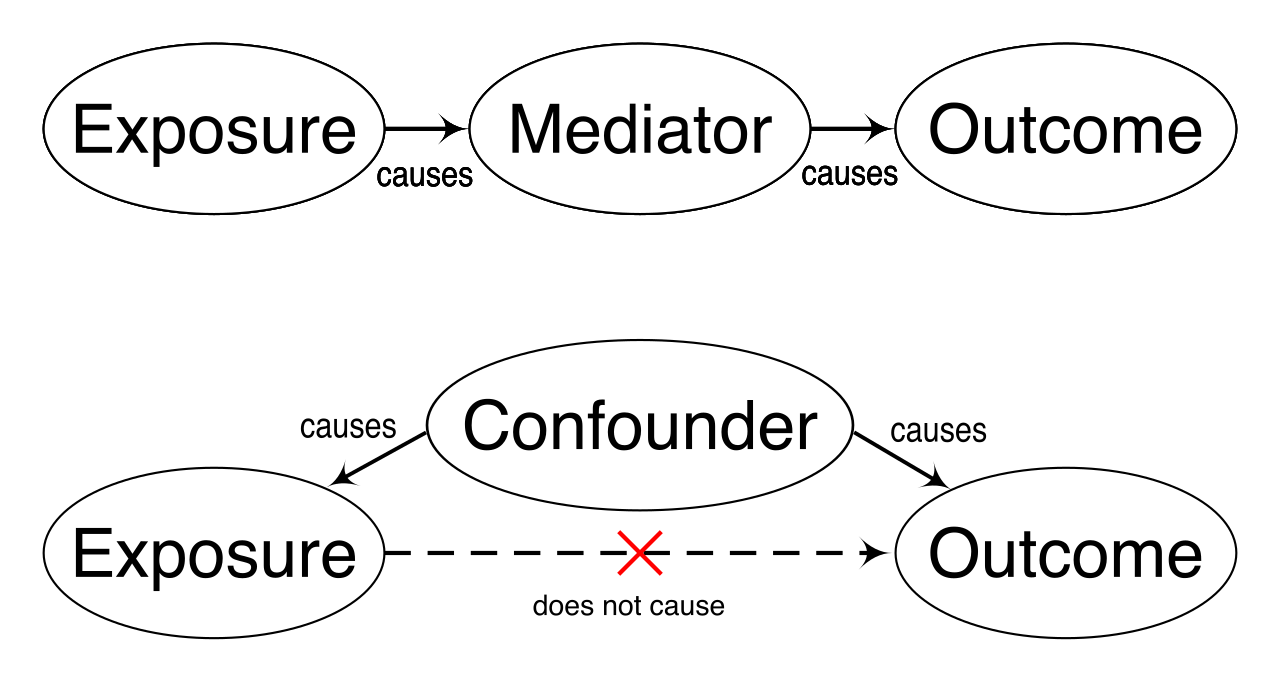
- Internal validity determines whether the observed changes in the dependent variable are truly caused by the independent variable. (Did your dressing actually prevent the infection, or was it just because the hospital also secretly changed the hand-washing soap?)
- External validity refers to the extent to which research findings can be generalized to a broader population. (If an intervention worked in a specialized oncology ward in New York, will it work in a general pediatric ward in Dammam?)
To protect patients from flawed science, nurses perform critical appraisal, which is the systematic evaluation of clinical research papers to establish study validity and clinical relevance. Several standardized tools guide this process:
- The CASP checklist is a widely used tool for critically appraising the strengths and limitations of published research studies.
- The PRISMA statement is an evidence-based minimum set of items used for reporting systematic reviews and meta-analyses. It ensures authors are transparent about how they selected their data.
- The AGREE II instrument is a globally recognized tool used to evaluate the methodological quality of clinical practice guidelines.
History is scarred by research that violated human rights. Today, strict ethical guardrails protect participants. Institutional Review Boards (IRBs) must approve nursing research proposals to ensure the protection of human subjects before data collection begins.
Research ethics are anchored in universal principles:
- Beneficence: The ethical principle of beneficence in research requires researchers to maximize potential benefits and minimize potential harms to participants.
- Autonomy: The ethical principle of autonomy requires researchers to obtain voluntary informed consent from all participants.
- Informed consent ensures participants understand the research purpose and associated risks before agreeing to participate.
- Withdrawal: Research participants possess the ethical right to withdraw from a study at any time without facing negative consequences. If a patient decides midway through a trial that they no longer wish to participate, their clinical care must not be compromised.
We must also meticulously guard patient information:
- Anonymity in research occurs when even the researcher cannot link a participant's identity to the provided data. (e.g., An unnumbered, drop-box survey).
- Confidentiality in research requires the researcher to securely protect known participant identities from public disclosure. (e.g., The researcher has the patient's medical record but uses a pseudonym in the published paper).
Why doesn't every nurse practice perfectly based on the latest evidence? Because the real world is chaotic. A primary organizational barrier to implementing evidence-based practice is the lack of dedicated time for nurses to read research literature.
However, organizations can construct bridges over these barriers. The presence of advanced practice nurses and clinical mentors facilitates the adoption of evidence-based practice on hospital wards. Furthermore, units often host journal clubs, which are collaborative meetings where nurses critically appraise recent research articles to enhance clinical knowledge.
When best practices are solidified, organizations create clinical practice guidelines, which provide evidence-based recommendations developed by expert panels to standardize nursing care. Instead of each nurse guessing the best way to treat a diabetic foot ulcer, the guideline provides a scientifically validated roadmap.
Research vs. Quality Improvement
Do not confuse research with quality improvement (QI). As stated earlier, research generates generalizable knowledge. By contrast, quality improvement initiatives aim to improve specific internal work processes within a single healthcare facility.
If you are trying to figure out why the medication administration process on your specific ward in Riyadh is delayed and how to speed it up, you are doing QI. Because QI is internally focused and poses minimal risk, quality improvement projects generally do not require approval from an Institutional Review Board.
Final Thought for the SNLE: When you sit for the exam, visualize the clinical reality. EBP is not a dusty textbook concept. It is the synthesis of top-tier literature, your sharp clinical judgment, and the profound cultural values of the patient sitting in front of you. By understanding how to formulate a PICOT question, evaluate an RCT's internal validity, and deploy an EBP intervention ethically, you are protecting patients and elevating the entire profession of nursing.