Pharmacology
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
When a chemical substance is introduced into the human body, a profound and intricate physical dialogue begins. On one side, the body acts mechanically upon the molecule—dissolving it, transporting it across lipid bilayers, altering its chemical structure, and ultimately flushing it out. On the other side, the molecule acts upon the body, locking into microscopic cellular receptors to alter the heartbeat, silence a pain signal, or lower blood pressure. In clinical practice, mastering this dialogue is not a theoretical exercise; it is the fundamental barrier between a therapeutic cure and a catastrophic systemic failure. To prepare for the rigors of the Saudi Nursing Licensure Examination (SNLE) and your subsequent practice in high-acuity wards across the Kingdom, you must understand both the invisible mechanics of these drugs and the uncompromising legal and safety frameworks that govern their administration.
To understand pharmacology, we must divide our thinking into two distinct but permanently linked scientific disciplines: what the body does to the drug, and what the drug does to the body.
Pharmacokinetics is the study of how a drug moves through the body over time. It is purely a matter of transit and processing, governed by four distinct phases: absorption, distribution, metabolism, and excretion.
Conversely, pharmacodynamics is the study of the biochemical and physiological effects of drugs on the body. Once the drug arrives at its destination, pharmacodynamics explains how it actually works.
Phase 1: Absorption and the First-Pass Effect
Absorption is the journey of the drug from its site of administration into the systemic circulation. The rate of drug absorption directly determines the onset of the medication's action. If you give a patient an oral tablet, it must survive the harsh acidic environment of the stomach, pass into the small intestine, and cross the intestinal wall into the portal vein.
However, before this oral drug ever reaches the systemic circulation to do its job, it must flow through the liver. Here, the liver acts as a heavy-handed toll collector in a phenomenon known as the first-pass effect, which significantly reduces the bioavailability of orally administered medications. A large percentage of the active drug is destroyed before it can even reach the heart to be pumped to the rest of the body.
How do we bypass this toll collector? By changing the route.
- Intravenous medication administration entirely bypasses the absorption phase. Because the drug goes directly into the vein, intravenous administration results in one hundred percent bioavailability of the drug.
- Alternatively, the sublingual route requires placing a prescribed medication directly under the tongue for rapid systemic absorption. The rich capillary bed under the tongue drains directly into the superior vena cava; therefore, sublingual medication administration successfully bypasses the hepatic first-pass effect.
- Similarly, the buccal route requires securely placing a prescribed medication precisely between the patient's cheek and gum, utilizing the same principle of transmucosal absorption.
Phase 2: Distribution and the Protein-Binding Trap
Once in the blood, the drug must be distributed to the tissues. But the bloodstream is not just an empty river; it is filled with plasma proteins, primarily albumin. Many drugs act like passengers trying to board a specialized transit system—they bind tightly to albumin.
Here is the critical catch: Medication protein binding severely restricts drug distribution because only completely unbound drug molecules can exert a physiological pharmacological effect. The bound molecules are trapped in the bloodstream, inactive.
Geriatric Consideration: As we age, our physiological reserves diminish. Decreased serum albumin levels in elderly patients drastically increase the proportion of unbound, active drug molecules in the bloodstream. If an elderly patient takes a highly protein-bound drug but lacks the albumin to hold it, a massive wave of unbound drug is unleashed, leading to sudden toxicity.
Phase 3 & 4: Metabolism, Excretion, and the Half-Life
Eventually, the drug must be neutralized and removed.
- The liver is the primary physiological site of drug metabolism. It breaks down the active molecule into inactive, water-soluble metabolites.
- The kidneys serve as the primary organs for drug excretion from the body, filtering these water-soluble metabolites into the urine.
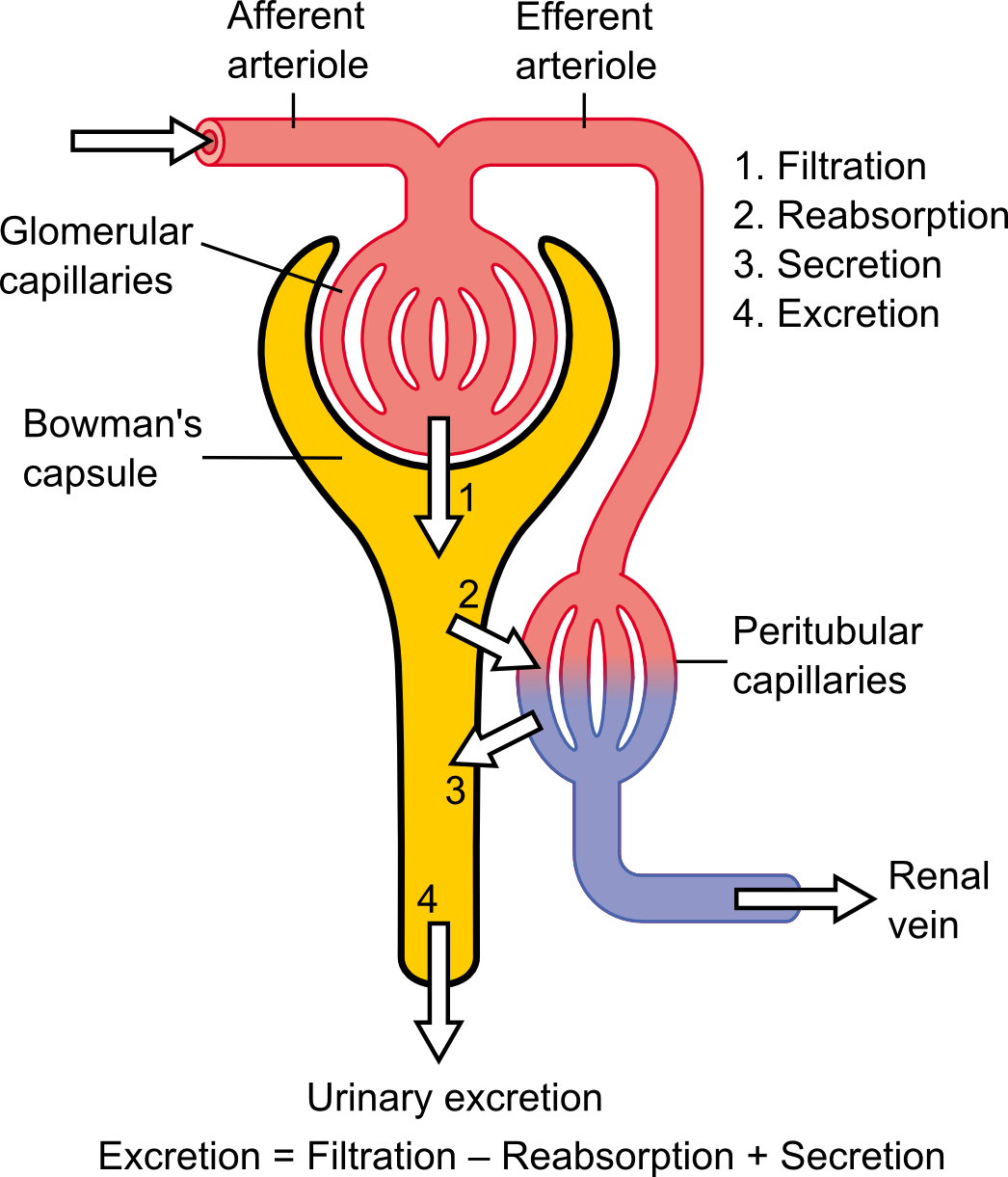
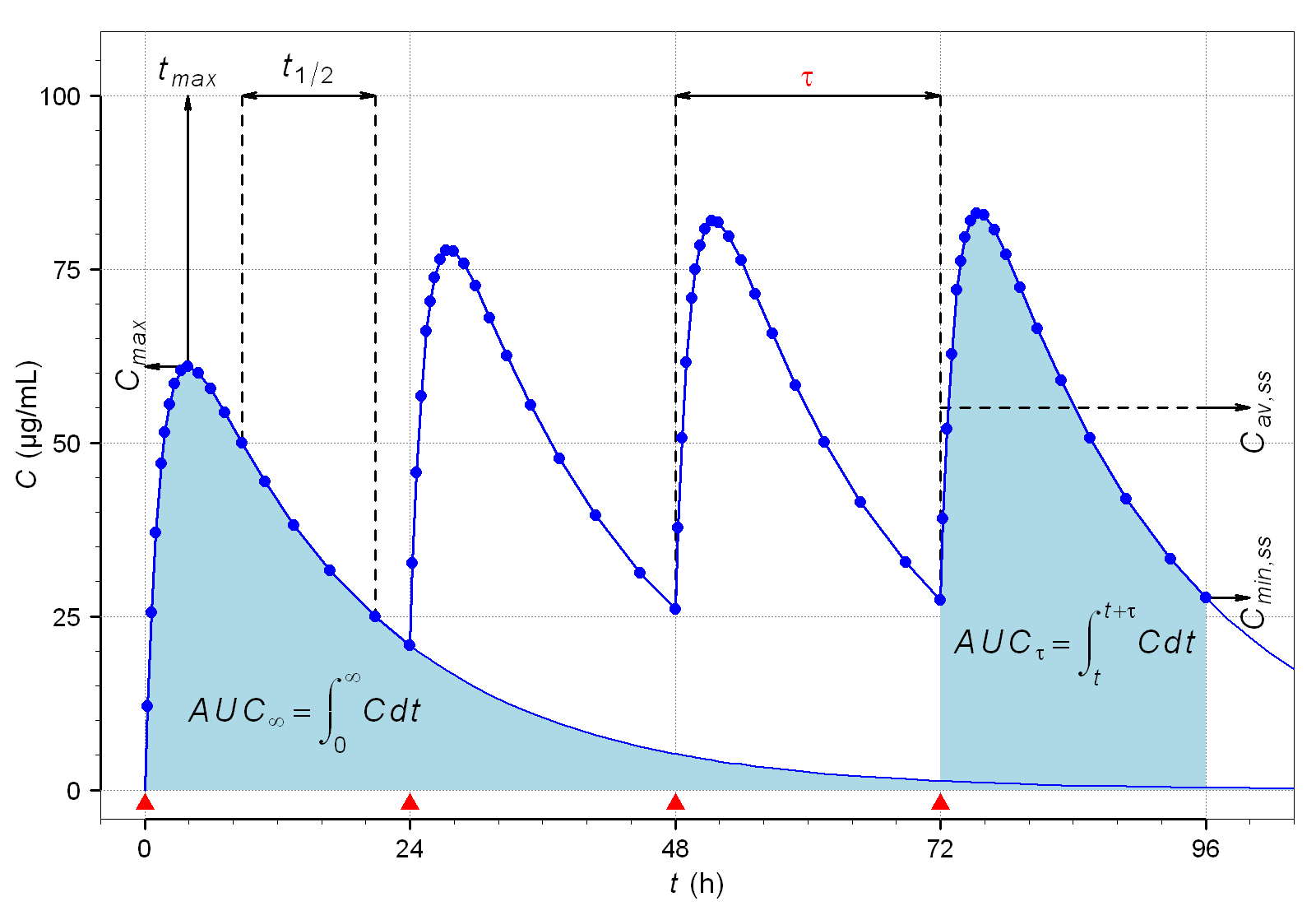
Because these two organs are the cleanup crew, organ failure dramatically changes drug kinetics. Hepatic impairment prolongs the half-life of many hepatically metabolized medications. Speaking of which, half-life is the specific time required for the total concentration of a drug in the body to decrease by exactly fifty percent.
If the kidneys fail, the exit door is locked. Renal impairment severely increases the risk of drug toxicity due to delayed excretion. Because of the normal age-related decline in renal function, geriatrics mandates significantly lower starting doses of renally excreted medications.
Metabolic Interactions
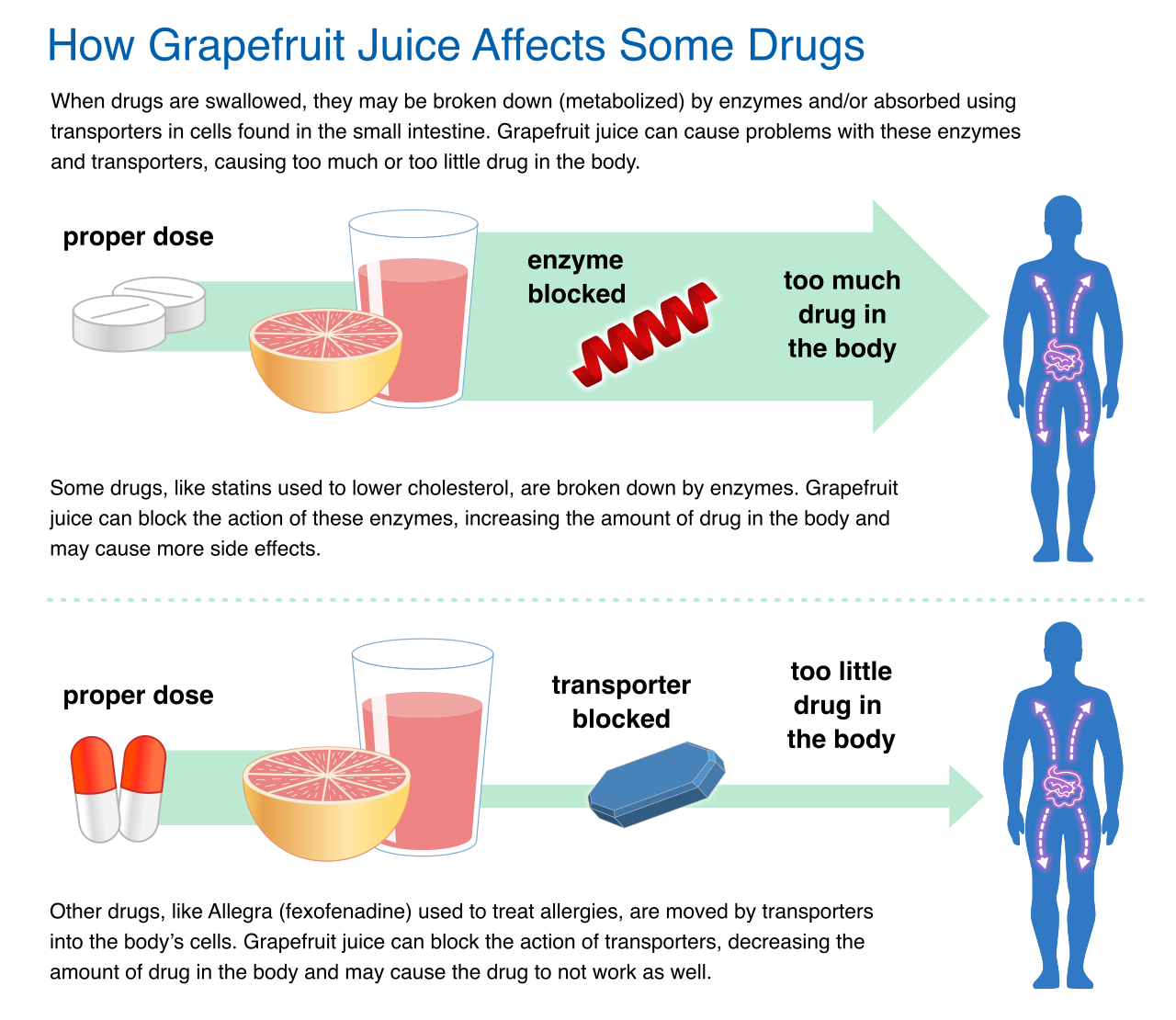
Sometimes, the food we eat hijacks our metabolic machinery. A classic SNLE scenario involves the CYP3A4 enzyme in the liver, a major processor of statins and calcium channel blockers. Ingesting grapefruit juice significantly inhibits the natural function of the CYP3A4 metabolic liver enzyme. By paralyzing the cleanup crew, inhibiting the CYP3A4 metabolic liver enzyme dangerously increases the total systemic bloodstream concentration of certain oral medications.
Once the drug reaches the target cell, it interacts with cellular receptors in one of two ways:
- An agonist medication binds directly to a cellular receptor to produce a biological response. (It turns the cellular switch on).
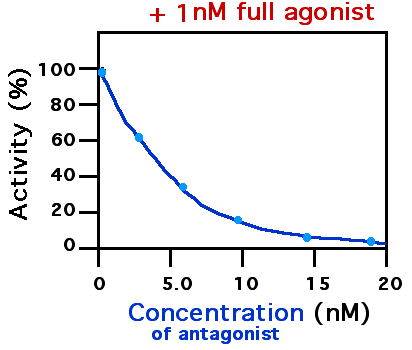
- An antagonist medication binds directly to a cellular receptor to block an expected biological response. (It jams the lock so nothing else can turn the switch).
The Therapeutic Index
Not all drugs are forgiving. The therapeutic index is the calculated ratio between a drug's toxic dose and its clinically effective dose.
- A wide therapeutic index means there is plenty of room for error.
- Drugs possessing a narrow therapeutic index require routine and frequent serum level monitoring. The difference between a cure and a lethal overdose is razor-thin (e.g., Digoxin, Vancomycin).
To monitor these dangerous drugs, we draw blood to measure peaks and troughs:
- Peak drug levels represent the absolute highest concentration of a specific drug in the patient's bloodstream. Because absorption times vary by route, peak levels are drawn at a specific prescribed interval after medication administration depending entirely on the drug's route.
- Trough drug levels represent the absolute lowest concentration of a specific drug in the patient's bloodstream. To ensure we don't accidentally stack a new dose on top of an uncleared old dose, trough levels are routinely drawn immediately before administering the next scheduled medication dose.
The Spectrum of Drug Response
Over time, the body adapts to the presence of a drug, presenting three distinct clinical phenomena:
- Pharmacological tolerance manifests as a progressively decreased physiological patient response to a specific medication following repeated clinical administration. (The patient needs a higher dose to achieve the same pain relief).
- Physical drug dependence is a profound physiological adaptation to a specific medication that immediately produces clinical withdrawal symptoms upon sudden cessation. (The cellular machinery has rewired itself to expect the drug).
- Psychological drug addiction is uniquely characterized by compulsive, uncontrollable medication use despite devastating personal and medical consequences. (This is a behavioral and neurobiological pathology).
In the ward, you are the final line of defense before a chemical enters the patient.
The six standard rights of medication administration are right patient, right drug, right dose, right route, right time, and right documentation.
To ensure the "right patient," verifying the right patient safely requires the use of at least two independent patient identifiers. By universal standard, standard acceptable patient identifiers include the patient's full name and the assigned medical record number. Never use environmental markers; a patient's hospital room number is strictly prohibited as a patient identifier, as patients are routinely moved or transferred.
High-Alert Medications: The PINCH Acronym
Certain drugs are fundamentally more dangerous. High-alert medications carry a significantly elevated risk of causing devastating patient harm when administered incorrectly.
The PINCH acronym outlines common high-alert medications requiring strict safety protocols:
Because the margin for error is zero, independent double-checking protocols require two distinct nurses to separately calculate and verify a high-alert medication dose. You do not check together; you calculate independently and compare results to strip away confirmation bias.
LASA and the Polypharmacy Risk
Many errors stem from visual and auditory cognitive failures. The healthcare acronym LASA designates Look-Alike, Sound-Alike medications (e.g., DOBUTamine vs. DOPamine). To break visual uniformity, Tall Man lettering is a specialized typographical technique utilized to visually distinguish Look-Alike, Sound-Alike medications from one another.
Drug interactions are a massive threat, particularly in geriatrics. Polypharmacy profoundly increases the statistical risk of adverse drug interactions in the elderly patient population.
The way a drug is physically manufactured dictates exactly how you must administer it. Violating these rules destroys the drug's pharmacokinetic design.
Oral Formulations
- Enteric-coated tablets must never be crushed under any circumstances. These are designed to bypass the stomach and dissolve in the intestines. Crushing an enteric-coated tablet prematurely destroys its crucial protective gastric layer, exposing the stomach mucosa to intense irritation or destroying the drug in stomach acid.
- Extended-release capsules must never be chewed by the patient. They contain a massive 12-to-24-hour dose designed to leak slowly. Chewing an extended-release capsule immediately triggers rapid systemic absorption of a potentially toxic medication dose.
Topical and Transdermal
- Transdermal medication patches must be firmly applied to clean, completely hairless skin to ensure consistent transdermal absorption.
- Nurses must systematically rotate transdermal patch application sites to effectively prevent localized skin irritation.
- Crucially, to prevent an unintended overdose, old transdermal medication patches must be completely removed from the patient before applying a new prescribed patch.

Ophthalmic and Otic Drops
- Ophthalmic medication drops must be carefully instilled directly into the patient's lower conjunctival sac, never directly onto the sensitive cornea. Furthermore, applying gentle, sustained pressure to the nasolacrimal duct immediately after eye drop instillation effectively prevents unintended systemic medication absorption.
- For the ear, anatomy dictates your technique:
- When administering otic drops to an adult patient, the ear pinna must be pulled firmly up and back to properly straighten the ear canal.
- When administering otic drops to a child under three years old, the ear pinna must be pulled gently down and back to properly straighten the ear canal.

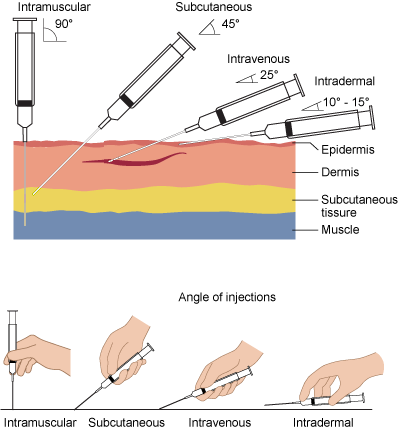
Parenteral Routes (IM and IV)
For deep muscle injections, the ventrogluteal site functions as the preferred intramuscular injection site for adult patients due to its minimal risk of underlying nerve injury. If you use the arm, remember that the deltoid muscle can safely and effectively accommodate a maximum intramuscular injection volume of exactly one milliliter. To protect the tissue during IM delivery, the Z-track injection method is specifically utilized for intramuscular injections to safely prevent medication leakage into surrounding subcutaneous tissue.
Intravenous therapy removes all physiological barriers. Intravenous bolus medication administration inherently carries the highest overall risk for immediate adverse effects due to its exceptionally rapid systemic delivery. You must monitor the IV site constantly to distinguish between three distinct localized complications:
| IV Complication | Clinical Definition |
|---|---|
| Infiltration | Intravenous infiltration definitively occurs when non-vesicant intravenous fluid accidentally leaks directly into the surrounding local tissue. (Cool, swollen, pale). |
| Extravasation | Intravenous extravasation definitively occurs when a vesicant medication leaks directly into surrounding local tissue and causes subsequent cellular necrosis. (Tissue death, blistering—a clinical emergency). |
| Phlebitis | Phlebitis is the localized inflammation of a vein directly caused by chemical, bacterial, or mechanical irritation originating from intravenous therapy. (Red, warm, cord-like vein). |
There is a strict clinical distinction between side effects and adverse events.
- A medication side effect is a known, secondary, and typically undesirable effect of a specific pharmacological treatment (e.g., nausea from oral antibiotics).
- An adverse drug event encompasses any unexpected, unintended, or dangerous reaction resulting from a medication (e.g., Stevens-Johnson syndrome).
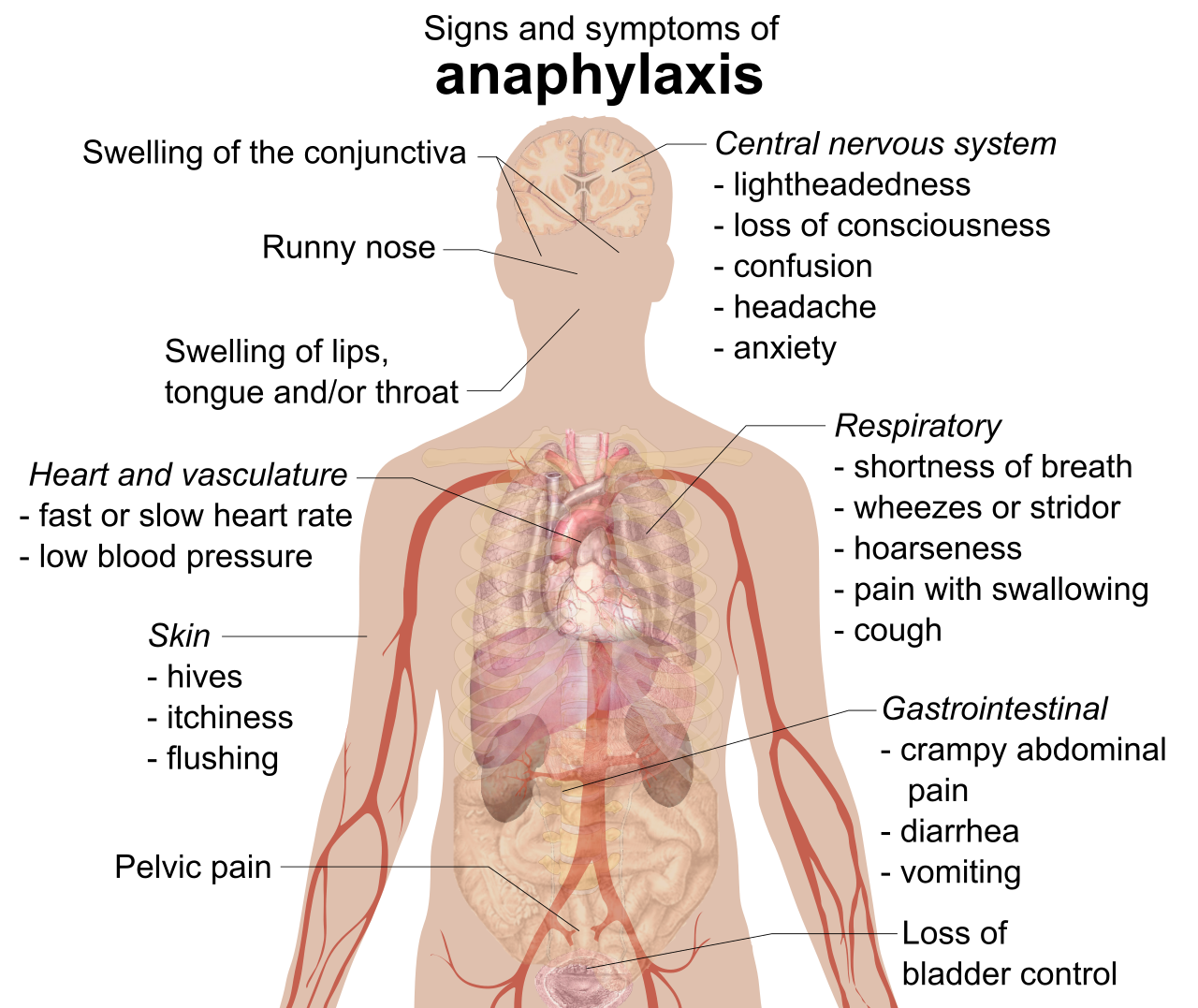
The most severe adverse event is an allergy. Nurses are strictly required to verify patient drug allergies immediately prior to administering any new clinical medication. If a patient experiences an extreme reaction, they are experiencing anaphylaxis. Anaphylaxis is an acute, severe, life-threatening allergic reaction triggered by exposure to a specific medication. When the airway closes and blood pressure plummets, intramuscular epinephrine serves as the primary, immediate emergency treatment for medication-induced anaphylactic shock.
Patient Education and Communication
Patients must be active participants in their care. Comprehensive patient education regarding medications must include the medication name, intended purpose, exact dosage, and common side effects. Simply telling a patient is not enough; you must verify retention. The teach-back method represents a scientifically validated technique to accurately evaluate a patient's understanding of complex medication instructions.
Reconciliation and History
Care transitions (ER to ICU, ICU to Medical Ward) are prime opportunities for errors. Formal medication reconciliation protocols must occur at absolutely every clinical transition of patient care.
Medication reconciliation represents the formal process of directly comparing a patient's new medication orders against all medications the patient has actively been taking. During this process, do not just ask about prescriptions. Routine over-the-counter medications and dietary herbal supplements must be explicitly included in the patient's formal medical history. Why? Because many common herbal dietary supplements can cause potentially dangerous drug-drug interactions when taken alongside prescribed pharmacological medications (e.g., St. John's Wort inducing CYP450 enzymes and destroying the efficacy of oral contraceptives).
Nursing documentation is a legally binding record of fact.
- Nurses must execute medication administration documentation immediately after the patient physically receives the drug.
- Documenting any medication administration before the patient actually consumes the drug constitutes a serious violation of nursing standards.
Medication Errors
If a failure occurs, transparency is paramount. An official incident report must be completed promptly following any clinical medication error. However, you must protect the facility's quality-improvement processes from legal discovery: The existence of an internal incident report regarding a medication error must never be documented within the patient's actual medical record. Document the facts of the patient's condition in the chart, but file the incident report entirely separately.
Verbal Orders
Physicians often give orders verbally, but this relies on auditory accuracy. Verbal medication orders must be directly transcribed into the medical record and explicitly read back to the prescribing physician. The rules tighten during a code blue: During emergency resuscitations, nurses must read back verbal medication orders aloud to confirm dosing accuracy prior to administration.
Patient Refusal and Placebos
Autonomy is a fundamental right. A patient's explicit refusal of any prescribed medication must be formally documented within the patient's permanent medical record. However, you cannot simply document "refused" and walk away. Nurses must actively explore and document the patient's underlying clinical reason for refusing a medication rather than simply accepting the refusal.
Never attempt to trick a patient. A clinical placebo is a completely inactive substance deliberately administered in a manner that perfectly mimics an active pharmacological medication. Using one deceptively is battery. Administering a placebo medication without first obtaining the patient's explicit informed consent directly violates foundational nursing ethical standards.
Finally, pharmacology relies on unyielding mathematics. The metric measurement system serves as the universal standard for calculating medication dosages across all healthcare environments.
You must commit the following volume conversions to memory:
- One liquid milliliter is exactly equivalent in volume to one cubic centimeter.
- One standard measuring teaspoon is precisely equivalent in volume to five fluid milliliters.
- One standard measuring tablespoon is precisely equivalent in volume to fifteen fluid milliliters.
Decimal Safety
A misplaced decimal point kills patients. The Joint Commission mandates strict typographical rules:
- A numerical leading zero must absolutely always be written immediately before a decimal point in written medication dosages (e.g., 0.5 mg, never .5 mg).
- A numerical trailing zero must absolutely never be written immediately after a decimal point in written medication dosages (e.g., 5 mg, never 5.0 mg, because a smudge makes it look like 50 mg).
Pediatric Dosing
Children are not simply miniature adults; their bodies have vastly different water-to-fat ratios and metabolic rates. Therefore, strict weight-based dosing calculations represent the mandatory standard clinical practice for all pediatric medication administration.
However, for the most toxic drugs on earth—chemotherapy—weight is not precise enough. Body surface area mathematical calculations consistently provide the most highly accurate medication dosing parameters for pediatric oncology patients, accounting for both metabolic mass and physical volume to ensure a perfect therapeutic strike against cancer cells.
In mastering pharmacology for the SNLE, recognize that you are not memorizing trivia. You are mastering the physics of medicine and the architecture of patient safety. Every rule, from the Z-track method to avoiding trailing zeros, exists because a failure in that exact mechanism previously cost a human life. Study the science, respect the rules, and protect your patients.