Quality and Safe Patient Care at the Frontline
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Imagine a modern healthcare facility not merely as a collection of beds and monitors, but as an immensely intricate, high-velocity machine. In this machine, hundreds of moving parts—nurses, physicians, pharmacists, complex devices, and critically ill patients—interact thousands of times a day. By the sheer laws of probability, things will eventually go wrong. The fundamental question of patient safety is not if errors will happen, but how we engineer the system to absorb, catch, and neutralize those errors before they ever reach the patient.
To master Quality and Safe Patient Care for the Saudi Nursing Licensure Examination (SNLE), you must stop viewing medical errors as the isolated failures of "bad" or "careless" nurses. Instead, you must look at the hospital as a physicist looks at a complex system. Every protocol, every barcode, and every double-check you perform on the ward is a mathematical probability filter designed to stop a chain reaction of failure.
In the past, healthcare operated under a culture of blame. If a nurse administered the wrong medication, the immediate reaction was to punish the nurse. However, modern healthcare relies on system effectiveness, a framework operating on the assumption that human errors are often symptoms of deeply flawed processes.
To understand this, we look at the Swiss Cheese Model of accident causation. Imagine stacking several slices of Swiss cheese together. Each slice represents a defensive layer in the hospital (e.g., electronic prescribing, pharmacy dispensing, nursing verification). The holes in the cheese represent vulnerabilities. For a catastrophic error to reach a patient, the holes in every single layer must momentarily align.
- Latent conditions are the hidden vulnerabilities embedded deep within the healthcare system design (e.g., understaffing, poorly designed software, or confusing policies).
- Active failures are the unsafe acts committed by personnel in direct contact with the patient (e.g., a nurse misreading a label).
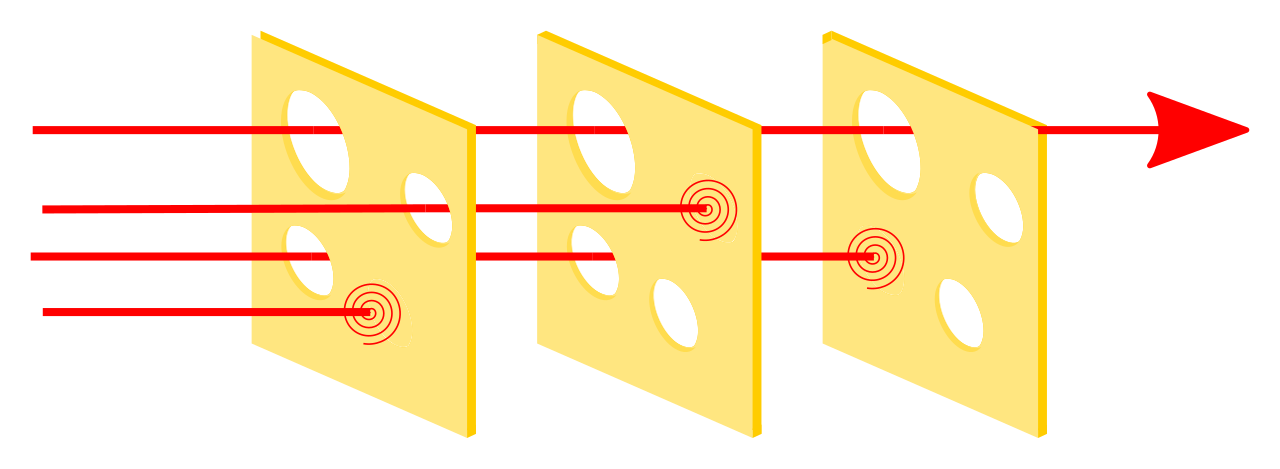
When we rely on redundant safety checks, we are essentially adding more slices of cheese to the stack. This minimizes the likelihood of a single human error reaching the patient.
Just Culture and the Danger of Workarounds
If we want to fix latent conditions, we must know they exist. This is the bedrock of a Just Culture, which encourages the reporting of clinical errors without fear of punitive action for unintended mistakes. A blame-free culture shifts the safety focus from individual errors to systemic vulnerabilities.
When processes are poorly designed, nurses often invent workarounds—informal clinical practices that intentionally bypass established safety procedures. While workarounds temporarily resolve immediate workflow obstacles for the clinical staff, they are deeply dangerous because they introduce undocumented and unmanaged risks directly to patient safety.
As you prepare to practice under the SCFHS, you must be intimately familiar with the regulatory authorities governing Saudi hospitals. The Saudi Central Board for Accreditation of Healthcare Institutions is the primary accrediting body for all healthcare facilities in Saudi Arabia.
Commonly known by the acronym CBAHI, this organization sets the gold standard for clinical operations. CBAHI enforces specific National Patient Safety Goals tailored for the Saudi healthcare context. Failing to meet these goals doesn't just mean poor patient care; it means a hospital can lose its accreditation to operate.
Communication breakdowns are the root cause of the vast majority of patient harm. Every time a patient's care is handed over from one provider to another, the risk of critical information being dropped skyrockets.
Handover Protocols
Implementing structured handover protocols vastly reduces communication breakdowns during critical shift changes. The gold standard is bedside shift reporting, which promotes patient safety by actively including the patient in the communication process. Furthermore, it provides the incoming nurse an opportunity to visually assess the patient immediately, confirming IV sites, dressings, and neurological baseline.
The SBAR Framework
When communicating critical information—especially when calling a physician about a deteriorating patient—nurses use the SBAR communication tool. This provides a standardized framework for sharing critical patient information among healthcare providers.
- S - Situation: What is happening right now? (e.g., "The patient is having acute respiratory distress.")
- B - Background: What is the relevant clinical history? (e.g., "He is day two post-op from a coronary bypass.")
- A - Assessment: What do I think the problem is? (e.g., "His oxygen saturation is 84%, and I hear crackles in the bases.")
- R - Recommendation: What do I need you to do? (e.g., "I need you to come evaluate him immediately and order a stat chest X-ray.")
Managing Orders and Critical Results
When a physician cannot enter an order electronically, you must rely on the verbal order read-back protocol. This requires the receiver to physically write down the prescribed order and then read the written order back to the prescribing physician for confirmation.
Similarly, CBAHI's National Patient Safety Goals mandate the immediate reporting of critical laboratory results within a strictly defined timeframe. When the lab calls you with a critical potassium level, the read-back protocol for critical laboratory values dictates that you must explicitly verify the patient's complete identity and repeat the exact quantitative test result to the caller to ensure absolute accuracy.
Administering medication is the most perilous high-wire act a nurse performs daily. To mitigate this, hospitals deploy several interconnected technological and procedural safeguards.
Patient Identification
Before you give a medication, draw blood, or perform a procedure, accreditation standards require the use of at least two patient identifiers (usually full name and Medical Record Number). Crucially, patient room numbers must never be used as a valid patient identifier, as patients are frequently moved.
High-Alert and Look-Alike Medications
High-alert medications (like insulin, heparin, and opioids) possess an inherently increased risk of causing significant patient harm when used in error. Because of this, independent double-checking by two licensed nurses is an essential safety requirement before administering them.
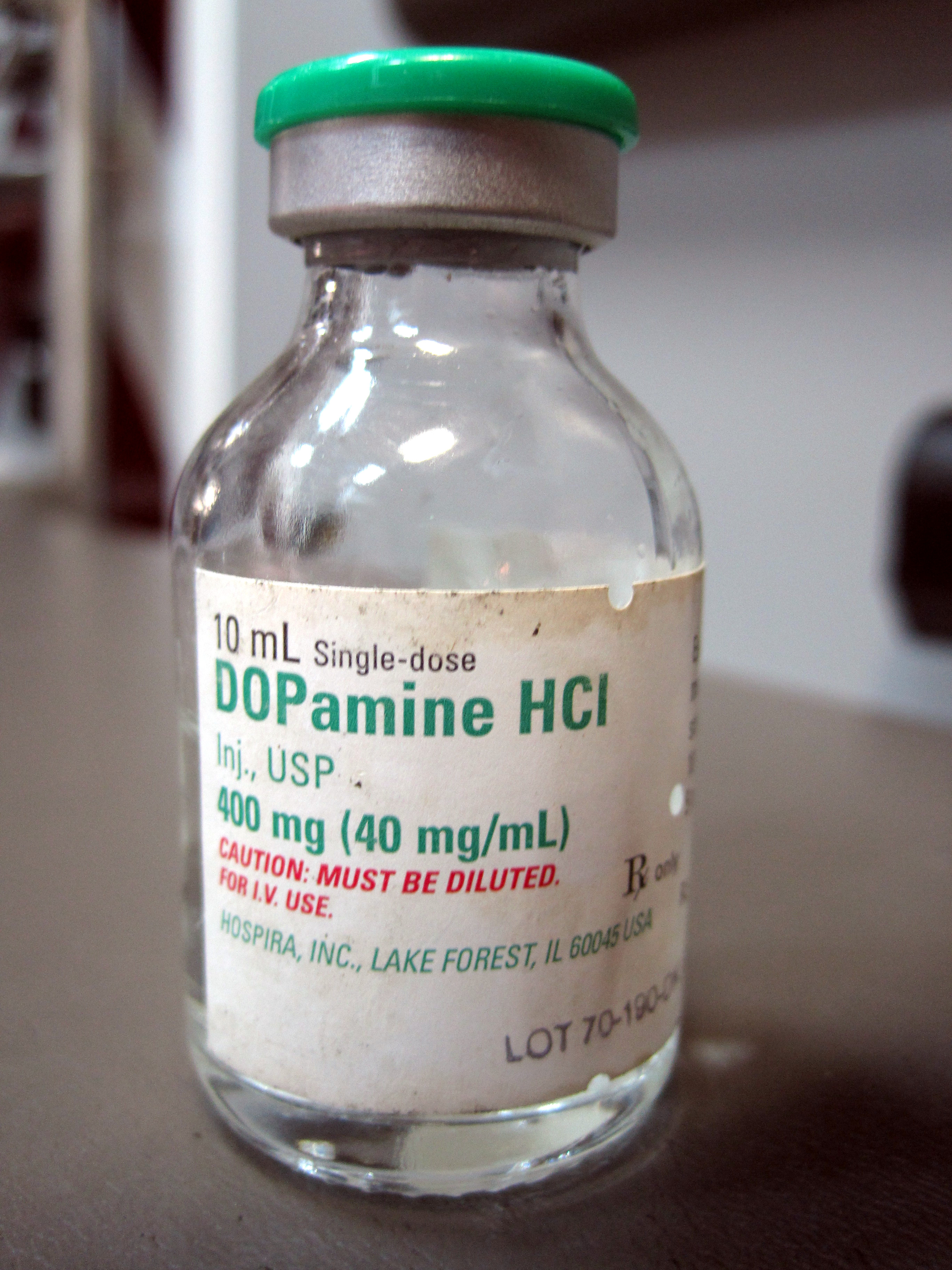
Furthermore, look-alike, sound-alike (LASA) medications are a frequent cause of catastrophic medication administration errors (e.g., confusing Dopamine with Dobutamine). To combat this, pharmacy systems utilize Tall Man lettering, which uses distinct uppercase letters to visually distinguish similar-looking medication names (e.g., DOPamine vs. DOBUTamine). This specifically helps prevent dispensing errors for look-alike medications in the pharmacy.
Technological Safeguards
At the bedside, Barcode Medication Administration (BCMA) systems digitally verify the patient's identity using an encoded wristband and confirm the scanned medication perfectly matches the electronic health record order.
Intravenous infusions carry their own risks. IV infusion pumps equipped with automated dose error reduction systems are referred to as smart pumps. Smart pumps utilize a built-in drug library with programmed hard and soft limits to prevent medication overdoses. Manually bypassing smart pump drug libraries entirely defeats the primary safety mechanism of the device.

Alarm Fatigue and Equipment Standardization
Our modern wards are filled with beeping machines. When nurses are exposed to a constant barrage of alarms, alarm fatigue occurs—they become desensitized to frequent clinical alarms on the unit. Alarm fatigue drastically increases the risk of nurses missing critical changes in a patient's physiological status. One way to mitigate the sheer overwhelm of clinical environments is the standardization of medical equipment across hospital units, which significantly reduces the cognitive load on nursing staff.
Protecting the Patient
CBAHI emphasizes proactive risk identification during routine daily nursing rounds. Certain clinical risks are ubiquitous and must be screened for aggressively:
- Fall Risk: Fall risk assessments must be conducted upon patient admission to identify individuals requiring specific safety interventions. The Morse Fall Scale is a widely used standardized tool to assess a patient's likelihood of falling.
- Pressure Injuries: Skin breakdown is devastating but largely preventable. The Braden Scale is a highly validated standardized risk assessment tool for predicting pressure injury risk.
- Medication Reconciliation: This is the systematic process of creating the most accurate list possible of all medications a patient is taking. It must occur at every transition of care (admission, transfer, discharge) to prevent adverse drug events.
Infection Control
Healthcare-associated infections (HAIs) are infections acquired by a patient while receiving care in a clinical facility. A major SNLE focus is on Catheter-associated urinary tract infections (CAUTIs), which are a primary focus of quality improvement initiatives to reduce hospital complications.
To combat HAIs, hospitals use bundles of care—groupings of evidence-based interventions that consistently result in better outcomes when implemented together. Similarly, standardized clinical protocols are employed to reduce undesirable variations in daily nursing practice.
Nothing beats proper hand hygiene. The World Health Organization outlines five specific moments for hand hygiene in healthcare settings. Remember the hierarchy: Alcohol-based hand rubs are the preferred method for routine hand hygiene when hands are not visibly soiled. However, handwashing with antimicrobial soap and water is strictly required when hands are visibly soiled (or when dealing with spore-forming bacteria like C. difficile).
Protecting the Procedure: The Universal Protocol
Surgery performed on the wrong body part is officially classified as a never event. Never events are severe, shockingly unacceptable medical errors that should not occur under any circumstances.
To prevent this, the Universal Protocol for preventing wrong-site surgery relies on three non-negotiable steps:
- A formal pre-procedure verification step.
- Marking the operative site with an unambiguous indicator.
- A mandatory clinical time-out immediately before starting the procedure. The surgical time-out must involve all immediate members of the procedure team communicating actively.
Protecting the Provider
You cannot pour from an empty cup. Ensuring healthcare provider safety is a fundamental prerequisite for maintaining consistent patient safety.
- Ergonomics: The utilization of safe patient handling equipment drastically reduces the risk of musculoskeletal injuries among nursing staff.
- Cognitive Sharpness: Fatigue management policies for nurses aim to decrease cognitive errors related to chronic sleep deprivation.
When the system fails, we must document and learn from it.
Internal tracking relies on Occurrence Variance Reports (also known as incident reports). These are internal documents used to track unexpected clinical events in a healthcare facility.
- They must contain objective descriptions of events without assigning personal blame.
- The primary operational purpose of an incident report is systemic quality improvement rather than individual staff discipline.
- An incident report must be completed immediately after the involved patient in a safety event is medically stabilized.
- Critical SNLE Rule: Occurrence Variance Reports are strictly internal quality tools and must never be documented or referenced in the patient's medical record.
Categorizing the Event
Near Miss: An unplanned patient safety event that did not result in actual injury to the patient. However, we do not ignore near misses; a near miss event highlights a critical system vulnerability with the potential to cause future patient harm.
Sentinel Event: A patient safety event resulting in death, permanent harm, or severe temporary harm. Sentinel events mandate an immediate administrative and clinical investigation.
Investigating the Event
How do we investigate? It depends on whether we are looking backward or forward.
| Tool | Approach | Purpose |
|---|---|---|
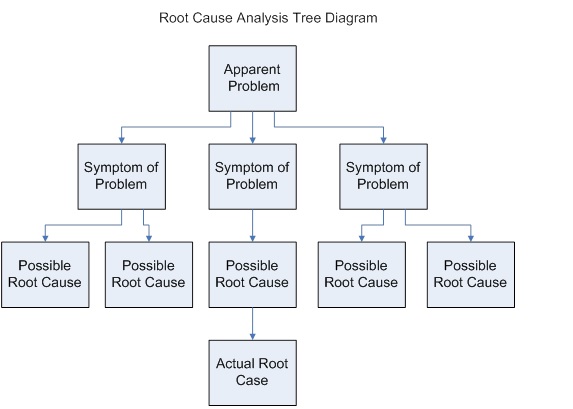
| Root Cause Analysis (RCA) | Reactive | A retroactive investigative process used to identify the underlying reasons for an adverse event. Note: Sentinel events require the completion of a formal Root Cause Analysis. |
| Failure Mode and Effects Analysis (FMEA) | Proactive | A risk assessment tool used to identify potential system failures before they occur. |
Quality improvement in nursing relies on continuous data collection to evaluate the outcomes of patient care.
To know if our nursing care is effective, we track nursing-sensitive indicators—specific metrics capturing clinical outcomes most directly affected by nursing practice. Patient fall rates serve as a primary nursing-sensitive quality indicator, alongside pressure injury prevalence, which is a universally tracked nursing-sensitive indicator.
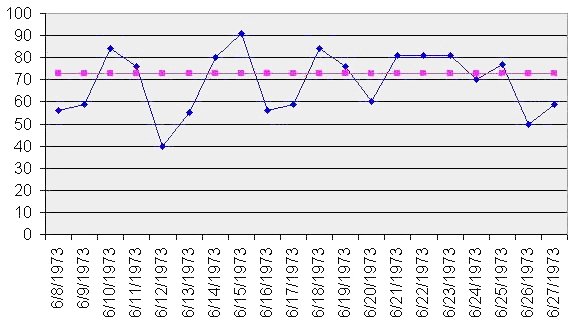
We measure success using Key Performance Indicators (KPIs), which are quantifiable measurements used to evaluate the success of quality improvement initiatives. To know if our KPIs are actually "good," we use benchmarking, which involves comparing a hospital unit's performance metrics directly against recognized industry standards. We then use run charts to graphically display this quality improvement data over time to identify trends in healthcare performance. To verify that actual frontline nursing care aligns with established clinical guidelines, units perform routine clinical audits by reviewing patient records.
Methodologies of Change
When the data tells us we need to change, we rely on established frameworks:
Lean vs. Six Sigma:
- Lean methodology in healthcare focuses heavily on eliminating process waste (e.g., removing unnecessary steps so a nurse doesn't walk two miles a shift just to fetch supplies).
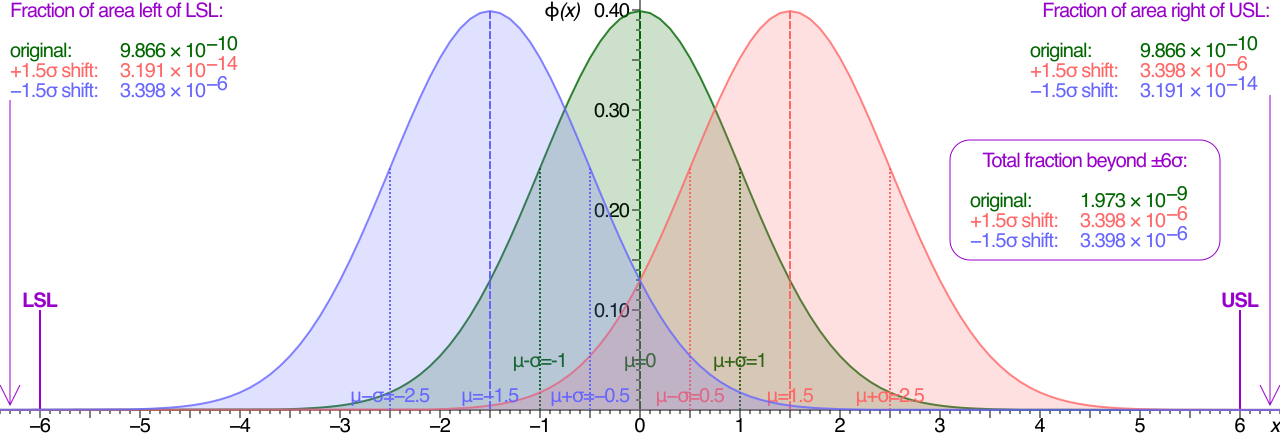
- Six Sigma methodology utilizes statistical analysis tools to reduce variation in healthcare processes (aiming for absolute, predictable uniformity).
The PDSA Cycle: The most widely used four-step model for implementing quality improvement changes on the unit is the Plan-Do-Study-Act cycle:
- Plan: Involves defining an objective for a specific healthcare improvement.
- Do: Involves implementing a proposed change on a small scale (e.g., trying a new handover sheet on one ward for one week).
- Study: Involves analyzing the data collected during the implementation phase to see if it actually worked.
- Act: Involves determining whether to formally adopt the tested change across the facility, abandon it, or tweak it and run the cycle again.
As you sit for the SNLE, remember: your role as a licensed nurse in Saudi Arabia is not just to be a compassionate caregiver at the bedside. You are the ultimate systems engineer of the ward, the final slice of Swiss cheese, and the primary guardian of patient safety.