Mental/Psychiatric Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Psychiatric nursing is fundamentally the science of translating profound, often chaotic human suffering into systematic clinical action. When you evaluate a patient in psychological distress, you are not merely cataloging eccentricities; you are mapping the neurochemical and structural breakdowns of the human mind. For the Saudi Nursing Licensure Examination (SNLE), mastery of this domain requires an analytical approach to assessment, an unwavering commitment to safe pharmacology, and the cultural intelligence to navigate psychiatric care within the context of the Saudi healthcare system.
The SNLE does not reward rote memorization of psychiatric definitions. It rewards the clinical judgment to know precisely when to listen, how to de-escalate, and why a particular intervention prevents a fatal outcome. Let us systematically break down the core competencies of mental and psychiatric nursing.
Before a nurse can intervene, they must accurately decode the patient's internal state. We achieve this through structured cognitive and behavioral assessments.
The Mental Status Examination (MSE)
Think of the Mental Status Examination as the physical assessment of the mind. It is a systematic framework that assesses a patient's appearance, behavior, speech, mood, affect, thought process, thought content, cognition, and insight.
To perform an accurate MSE, you must master the critical distinction between mood and affect:
- Mood represents a patient's subjective and pervasive emotional state. It is the climate of their internal world (e.g., a patient stating, "I feel hollow").
- Affect represents the clinician's observation of a patient's visible emotional expression. It is the daily weather (e.g., the nurse noting a patient is tearful or blunted).
For targeted cognitive evaluation, we use the Mini-Mental State Examination (MMSE), which is a widely used screening tool for cognitive impairment and dementia.
Decoding Perceptual and Thought Disturbances
Psychiatric pathophysiology frequently distorts a patient’s perception of reality. You must cleanly distinguish between these three phenomena:
- Hallucinations are abnormal sensory perceptions occurring without any external environmental stimuli (e.g., hearing voices in a completely silent room).
- Illusions are misinterpretations of real external sensory stimuli (e.g., seeing a highly coiled IV tubing and screaming that it is a snake).
- Delusions are fixed false beliefs that remain unchanged despite clear contradictory evidence.
Thought processes and speech can also derail, manifesting in specific, observable patterns:
- Flight of ideas: Rapid shifting from one topic to another with identifiable links between the topics.
- Word salad: A severely disorganized speech pattern consisting of a confused or unintelligible mixture of seemingly random words.
- Neologisms: Newly coined words or expressions created by a patient that have meaning only to the creator.
- Echolalia: The pathological, parrot-like repeating of words spoken by another person.
- Echopraxia: The involuntary imitation of the movements of another person.
In psychiatric nursing, your language is your primary procedural instrument. Therapeutic communication focuses entirely on advancing the physical and emotional well-being of the patient. It requires immense discipline.
Constructive Techniques
- Active listening: This involves fully concentrating on the patient's verbal and non-verbal messages. It is not passive hearing; it is an analytical engagement with the patient's presentation.
- Using silence: By intentionally utilizing silence, you provide the patient with necessary time to organize thoughts and process emotions.
- Reflecting: This technique directs the patient's questions and feelings back to the patient for self-exploration (e.g., Patient: "Should I leave my husband?" Nurse: "What do you think you should do?").
Destructive Patterns (Non-Therapeutic)
- Offering false reassurance: Stating "everything will be fine" minimizes the patient's concerns and disrupts the therapeutic nurse-patient relationship.
- Giving advice: Telling a patient what to do imposes the nurse's opinions on the patient and hinders the patient's ability to make independent decisions.
- Asking "why" questions: Demanding a rationale (e.g., "Why did you skip your medication?") can make a psychiatric patient feel defensive.
Clinical Protocol for Psychosis: When a patient experiences an active hallucination, the nurse must acknowledge the patient's feelings without validating the false perception ("I know you hear voices and that it is terrifying, but I do not hear them"). If a patient is delusional, arguing with a patient's delusion increases patient agitation and profoundly damages the therapeutic relationship. Instead, the nurse should focus on the underlying emotion of a delusion rather than the factual accuracy of the belief.
In Saudi Arabian culture, family involvement is deeply integrated into a patient's psychiatric treatment plan. The family unit often functions as a critical pillar of decision-making and recovery support.
Furthermore, cultural stigma surrounding mental illness often leads patients to present with somatic physical complaints (like chronic headaches or abdominal pain) instead of expressing emotional symptoms. A highly astute nurse recognizes that untreatable physical symptoms may veil a psychiatric crisis.
Finally, do not underestimate the power of faith. Muslim patients frequently utilize Islamic practices like prayer and reading the Quran as effective coping mechanisms during emotional distress. Facilitating these practices is not just culturally respectful; it is an evidence-based method of lowering patient anxiety.
The SNLE heavily tests your ability to adapt the nursing milieu (environment) to specific psychiatric pathologies.
Schizophrenia
Schizophrenia is characterized by a combination of positive, negative, and cognitive symptoms.
- Positive symptoms represent an addition of abnormal behaviors, including hallucinations and delusions.
- Negative symptoms represent a deficit of normal behaviors, including anhedonia (inability to feel pleasure), avolition (lack of motivation), and flat affect.
Mood Disorders: Depression and Bipolar Disorder
A Major Depressive Disorder diagnosis requires depressed mood or loss of interest for at least two consecutive weeks. Conversely, Bipolar I disorder is diagnosed when a patient experiences at least one full manic episode.
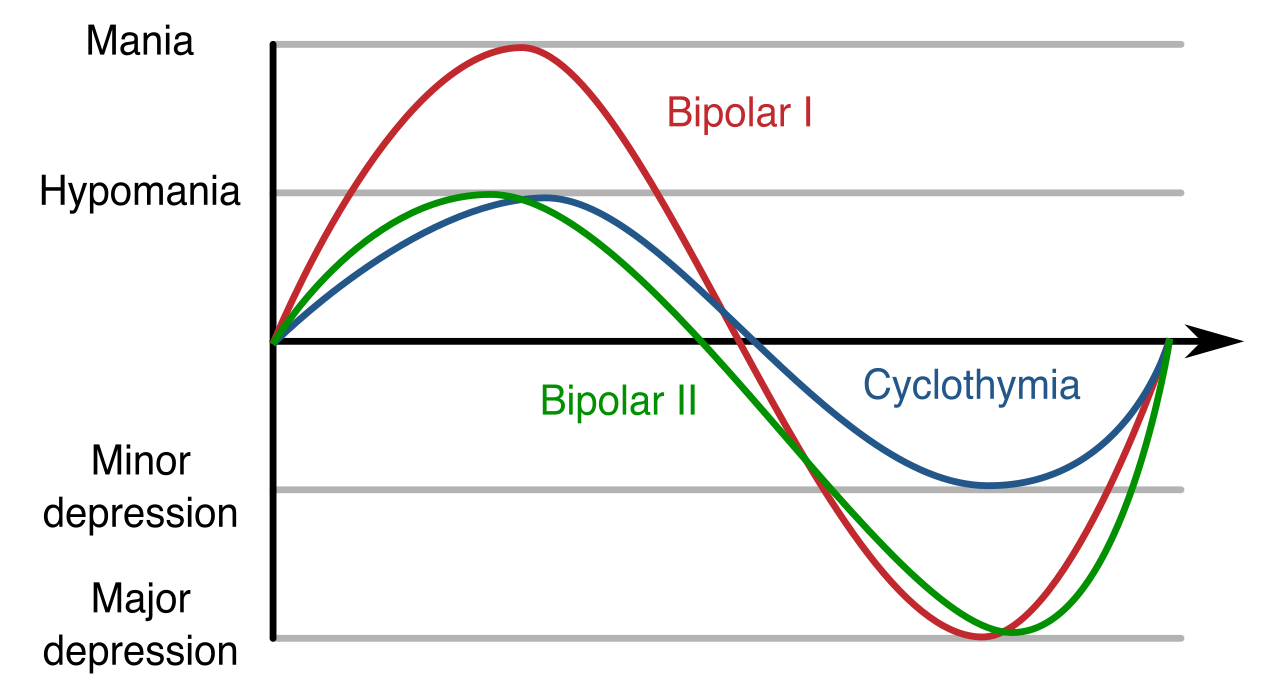
Mania involves an abnormally elevated mood, increased energy, and a decreased need for sleep.
- Milieu Control: The nurse must provide a safe, calm, and low-stimulus environment for a patient experiencing a manic episode.
- Nutrition: Because hyperactive manic patients rarely sit down to eat, they require high-calorie, high-protein finger foods to maintain nutritional status while moving.
Anxiety, Trauma, and Panic
- Obsessive-Compulsive Disorder (OCD) is characterized by intrusive thoughts causing profound anxiety (obsessions) and repetitive behaviors performed to reduce that anxiety (compulsions).
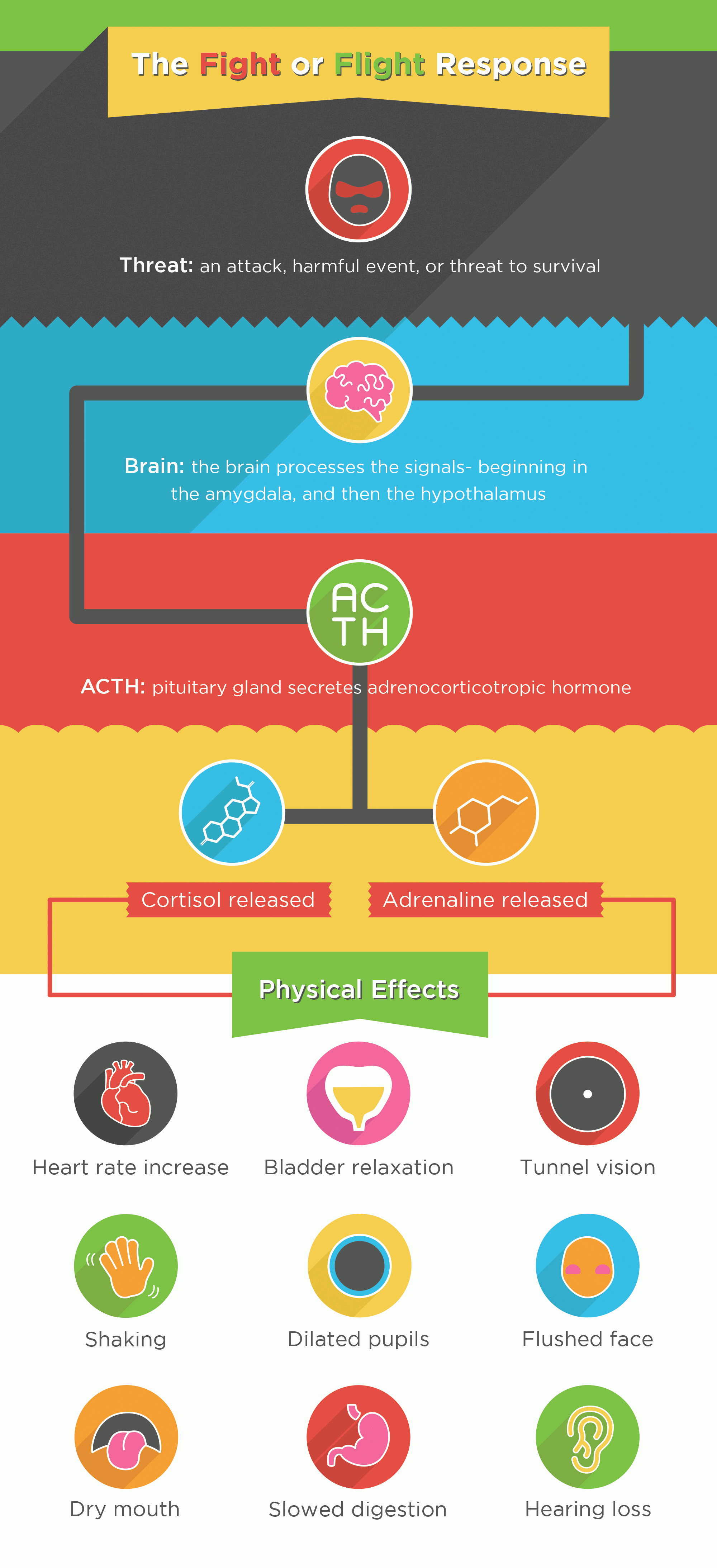
- Post-Traumatic Stress Disorder (PTSD) develops after exposure to a traumatic event. Symptoms include flashbacks, nightmares, and severe hyperarousal.
- Panic Disorder is characterized by recurrent, unexpected panic attacks. A panic attack involves an abrupt surge of intense fear reaching a peak within minutes. During a severe panic attack, the nurse must remain with the patient and use short, simple sentences. Complex instructions will not be processed.
Eating Disorders
- Anorexia nervosa involves an intense fear of gaining weight and a severely distorted body image.
- Bulimia nervosa is characterized by recurrent episodes of binge eating followed by compensatory purging behaviors (e.g., self-induced vomiting, laxative abuse). Critically, patients with bulimia nervosa are at high risk for severe electrolyte imbalances like hypokalemia, which can precipitate fatal cardiac arrhythmias.

Personality Disorders
- Borderline personality disorder involves severe emotional instability, impulsivity, and an intense fear of abandonment.
- Antisocial personality disorder is characterized by a pervasive disregard for the rights of others, often involving deceit, manipulation, and a lack of empathy.
Psychiatric medications carry extremely narrow margins for error. The SNLE will test your vigilance regarding lethal toxicities and side effects.
Antidepressants
- Selective Serotonin Reuptake Inhibitors (SSRIs) are a first-line pharmacological treatment for clinical depression. However, an overdose or interaction can cause Serotonin syndrome, a potentially life-threatening condition caused by excessive serotonergic activity in the nervous system. Symptoms include altered mental status, autonomic hyperactivity (fever, diaphoresis), and neuromuscular abnormalities (tremors, hyperreflexia).
- Monoamine Oxidase Inhibitors (MAOIs) interact dangerously with tyramine-rich foods (aged cheeses, cured meats). Consuming tyramine while taking MAOIs can trigger a severe hypertensive crisis.
Mood Stabilizers: Lithium
Lithium has a narrow therapeutic blood serum range of 0.6 to 1.2 mEq/L for maintenance therapy.
- Toxicity: Early signs of lithium toxicity include nausea, vomiting, diarrhea, and fine motor tremors.
- Electrolyte Balance: Because the kidneys cannot distinguish well between lithium and sodium, patients taking lithium must maintain consistent dietary sodium intake to prevent lithium toxicity. If a patient restricts sodium, the kidneys will reabsorb lithium, rapidly escalating blood levels to toxic ranges.
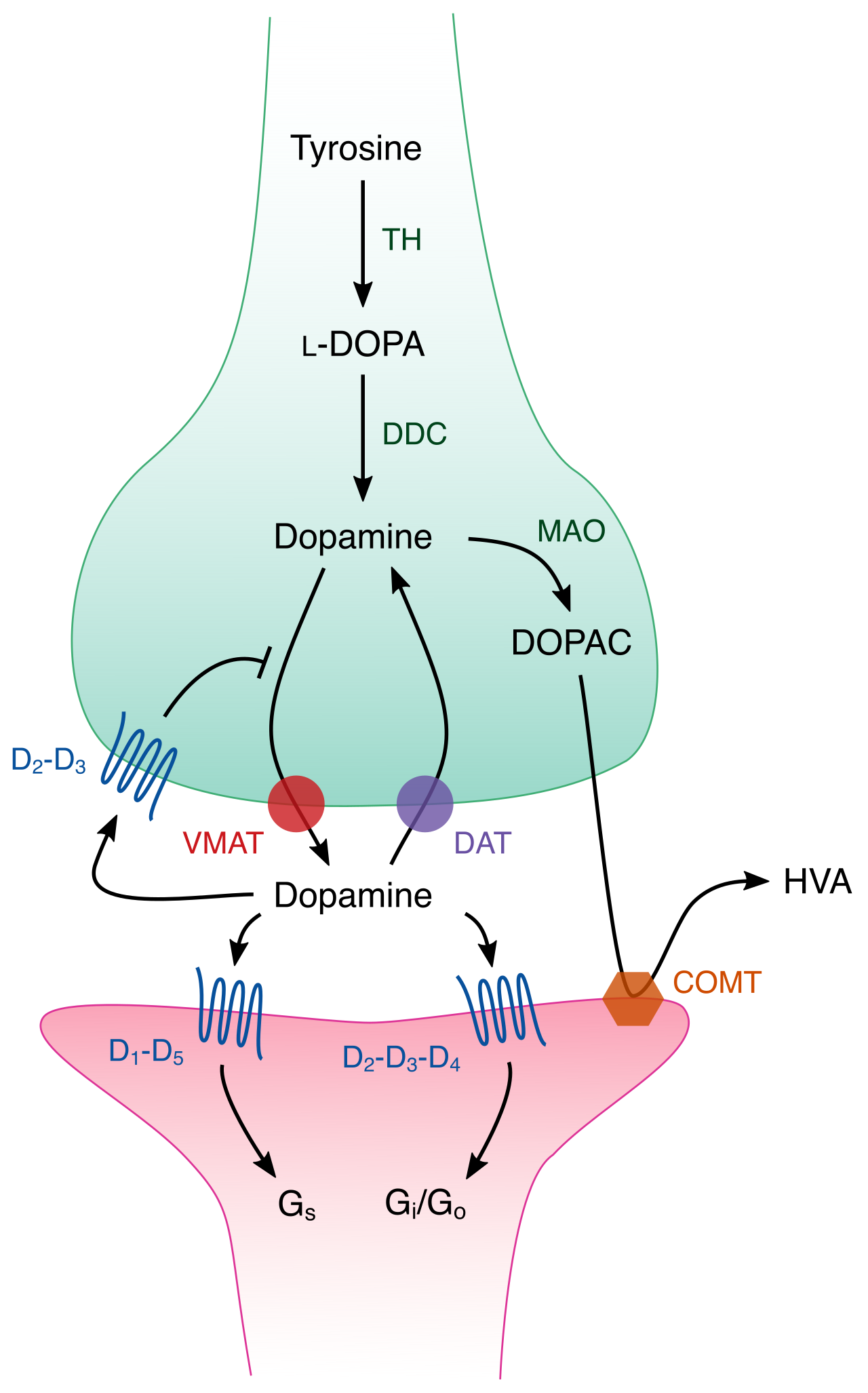
Antipsychotics
Typical antipsychotic medications frequently cause extrapyramidal side effects (EPS), which are movement disorders resulting from dopamine blockade. Recognize these distinct presentations:
- Acute dystonia: Involves involuntary muscle contractions of the face, neck, and back.
- Akathisia: Presents as an overwhelming internal sense of restlessness and an inability to sit still.
- Tardive dyskinesia: Involves irreversible, involuntary movements of the tongue, lips, and face.
Beyond EPS, typical antipsychotics can trigger Neuroleptic Malignant Syndrome (NMS). NMS is a rare, life-threatening reaction to antipsychotic medications that presents with severe muscle rigidity, high fever, and autonomic instability.
Atypical antipsychotics carry different risks. Clozapine is an atypical antipsychotic associated with a high risk of agranulocytosis (a severe drop in white blood cells). Consequently, patients taking clozapine require regular absolute neutrophil count (ANC) monitoring to detect this potentially fatal complication.
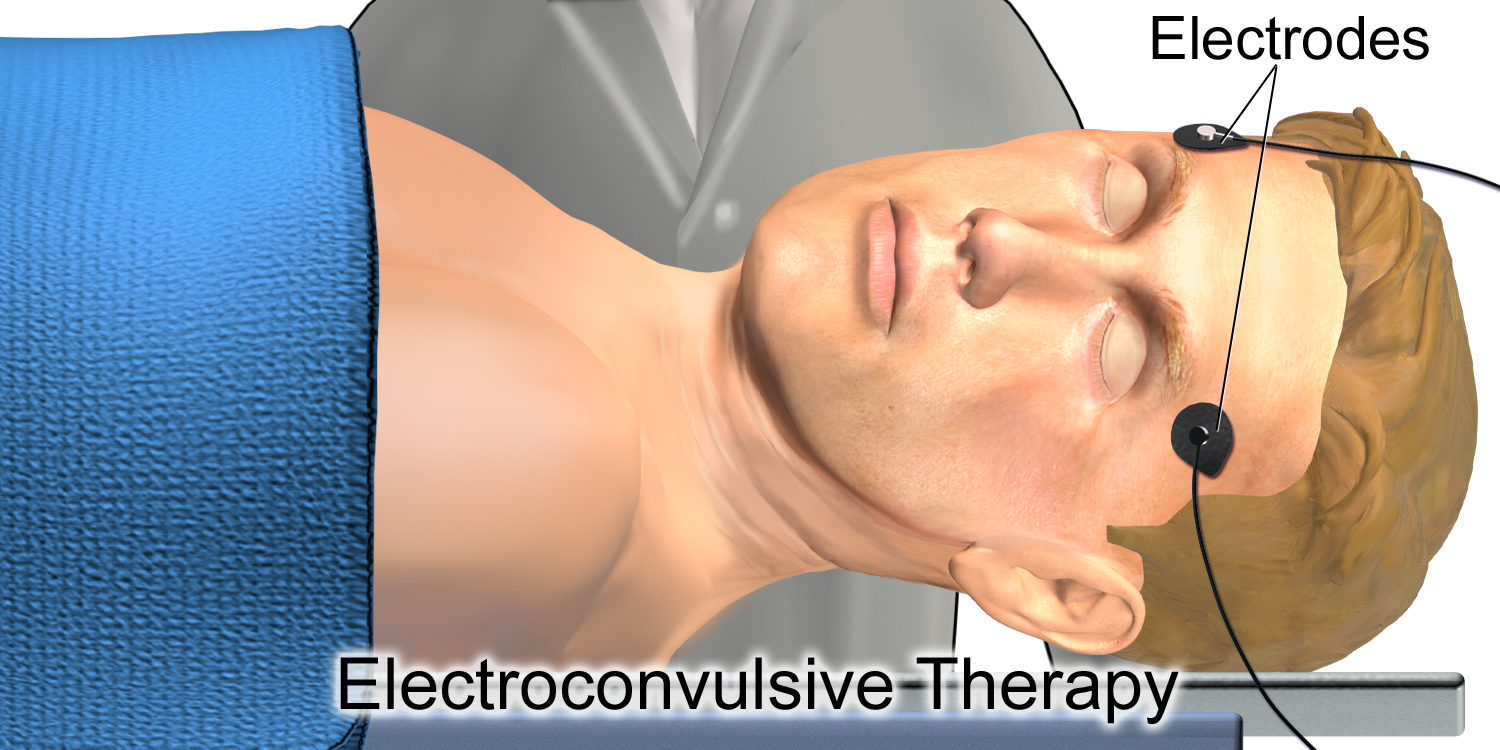
Electroconvulsive Therapy (ECT)
When pharmacology fails, Electroconvulsive therapy involves the intentional induction of a generalized seizure to treat severe psychiatric conditions.
- Pre-procedure: It requires informed consent and general anesthesia prior to the procedure.
- Post-procedure: The nurse must anticipate that temporary memory loss is a common and expected side effect of electroconvulsive therapy.
Patients naturally employ a defense mechanism—an unconscious psychological strategy used to cope with anxiety and protect the ego. Recognizing these helps decode a patient's behavioral presentation:
- Denial: Refusing to acknowledge an unpleasant reality or truth.
- Projection: Attributing one's own unacceptable thoughts or feelings onto another person.
- Displacement: Redirecting negative emotions from the original source to a safer, substitute target (e.g., a patient angry at the doctor yells at the nurse).
- Rationalization: Creating logical excuses to justify unacceptable behavior.
Transference and Countertransference
The emotional gravity of psychiatric care easily blurs interpersonal lines.
- Transference occurs when a patient unconsciously redirects feelings about someone in their past onto the nurse.
- Countertransference occurs when a nurse unconsciously redirects personal feelings onto the patient.
Maintaining strict professional boundaries is absolutely essential to manage countertransference in psychiatric nursing and ensure clinical objectivity.
In the ward, safety supersedes all other considerations.
Suicide Precautions
If a patient expresses active suicidal ideation, the intervention is absolute: a patient expressing active suicidal ideation requires immediate initiation of continuous one-to-one observation. Furthermore, the nurse must remove all potentially dangerous objects from the room of a suicidal patient.
Agitation and Restraints
When a patient escalates, de-escalation techniques prioritize verbal interventions and maintaining a non-threatening body posture.
If de-escalation fails, physical restraints are strictly utilized as a last resort when a patient poses an imminent danger to self or others. They are never used for convenience or punishment. Once restraints are applied, legal and ethical mandates dictate that nurses must assess skin integrity and circulation of restrained extremities at least every two hours.
Mastering these psychiatric nursing concepts does not merely ensure you pass the SNLE—it guarantees that when you walk onto a unit, you possess the clinical intellect to pull vulnerable minds back from the brink. Read the symptoms, anticipate the toxicities, and protect the patient.