Resources to Support and Coordinate Patient Care
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Imagine a high-acuity medical-surgical ward in Riyadh during the morning shift change. It is not merely a collection of beds, monitors, and medications; it is a highly complex, dynamic system constrained by time, personnel, and physical materials. Every time a nurse steps onto the unit, they are effectively managing a local economy of care. If resources—whether that means an infusion pump, a specialized nurse, or simply ten minutes of time—are allocated poorly, the entire system destabilizes. In the modern Saudi healthcare environment, a charge nurse or unit manager acts as the architect of this system, calculating inputs and balancing equations to ensure that every patient safely transitions from admission to discharge.

To master the Saudi Nursing Licensure Examination (SNLE), you must stop viewing management simply as administrative paperwork. Management and leadership functions in nursing are the fundamental physics of patient safety.
Before a single medication is administered, a unit must be staffed. Frontline resource planning involves anticipating the personnel required for a specific patient population as well as anticipating the materials required for a specific patient population. But how do we know what is required?
We do not staff units merely by counting beds; we staff them by calculating clinical complexity. Patient acuity systems classify patients according to the intensity of nursing care required. Because a critically ill patient demands vastly more clinical energy than a stable patient awaiting discharge, patient acuity is a primary determinant of nursing staffing needs on a hospital unit.
To codify this standard of safety, the Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI) requires hospitals to maintain a documented nurse staffing plan.
Staffing Math: FTEs and Working Hours
To build a schedule, managers calculate human capital in standardized units.
- A Full-Time Equivalent (FTE) is a standard measurement representing 40 hours of paid work per week.
- Importantly, one Full-Time Equivalent (FTE) position can be fulfilled by multiple part-time employees (for instance, two part-time nurses working 20 hours each equal 1.0 FTE).
Not all paid time translates to direct patient care. Managers must distinguish between:
- Productive hours: The paid time spent by nurses directly delivering patient care.
- Non-productive hours: The paid time nurses spend on vacation, sick leave, or educational training.
Skill Mix and Ratios
We must look beyond raw numbers. The nurse-to-patient ratio dictates the maximum number of patients assigned to a single nurse during a shift. However, ten novice nurses do not equal ten experienced specialists. Staffing effectiveness is determined by matching the competence of nursing staff with patient care needs.
This introduces the concept of skill mix. Skill mix refers to the proportion of registered nurses to other nursing personnel on a specific unit. The SNLE heavily tests this because it is a matter of life and death: a higher proportion of registered nurses in the skill mix is associated with lower patient mortality rates.
Staffing Systems: Control vs. Flexibility
Hospitals deploy different strategies to distribute these human resources, each with its own trade-offs:
| Staffing System | Mechanism | Primary Advantage |
|---|---|---|
| Centralized Staffing | A centralized staffing system involves a single administrative department making staffing decisions for all nursing units. | Centralized staffing generally provides greater cost control for the healthcare organization by eliminating overlapping inefficiencies. |
| Decentralized Staffing | A decentralized staffing system allows unit managers to create schedules based on specific ward needs. | Decentralized staffing generally provides greater scheduling flexibility for individual nurses, as managers understand local constraints. |
Predicting Demand and Covering Deficits
Healthcare is notoriously unpredictable, but we can manage the flow. Demand management involves predicting peak hospital admission times to ensure adequate nursing coverage.
When staffing deficits occur, hospitals rely on float pools, which consist of cross-trained nurses who provide temporary coverage for staffing shortages across various hospital units.
Clinical Warning: Never rely on forced labor to cover gaps. Mandatory overtime requires nurses to work beyond their scheduled shift to cover staffing deficits. The evidence is uncompromising: mandatory overtime is statistically associated with increased rates of clinical nursing errors and statistically associated with higher rates of nurse burnout. It is a failure of resource planning.
Once the staff is present, how is the work divided? Hospitals organize care using distinct delivery models:
- Functional Nursing: A care delivery model where specific clinical tasks are divided among different staff members (e.g., one nurse does all IVs, another does all wound care). It is efficient but fragments patient care.
- Team Nursing: Uses a registered nurse to lead a group of ancillary staff in providing care to a cohort of patients.
- Primary Nursing: **A care delivery model where one nurse assumes 24-hour accountability for a patient's care plan, from admission to discharge.
The Hub of Coordination
Regardless of the model, the registered nurse is the primary coordinator of care within a multidisciplinary healthcare team.
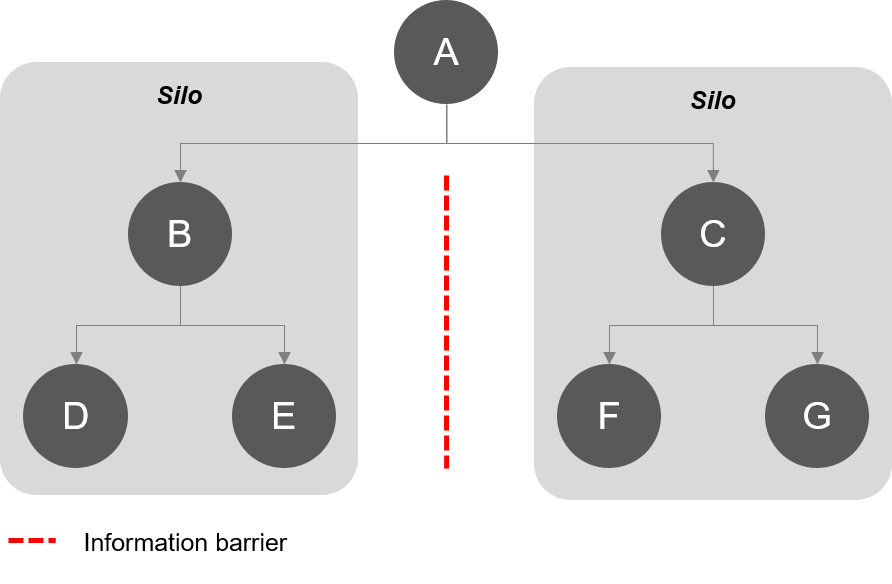
Care coordination involves organizing patient care activities among all participants to achieve safer care, and sharing information among all participants to achieve more effective care. Without coordination, the hospital acts as a set of disconnected silos. By fostering collaboration, we reduce waste; for example, effective interprofessional collaboration reduces the duplication of diagnostic testing for hospitalized patients.
One of the most effective tools for this is the rounding process. Multidisciplinary rounds improve patient care coordination by aligning treatment goals across different specialties—bringing the physician, nurse, pharmacist, and social worker to the same table.
Transitions and Trajectories
Patient care is a journey, not a snapshot. We utilize clinical pathways, which outline the expected sequence of multidisciplinary interventions for a specific diagnosis. Furthermore, these clinical pathways define the expected length of hospital stay for specific medical diagnoses.
To execute these daily, nurses use care maps, which integrate nursing care plans with multidisciplinary clinical pathways to guide daily care.
But human biology rarely follows a perfect script. Variances in a clinical pathway occur when a patient deviates from the expected progression of care (e.g., a post-op patient developing a sudden fever, delaying expected discharge).
When managing the overarching journey, case management focuses on optimizing patient outcomes across an entire episode of illness while simultaneously focusing on managing healthcare costs across an entire episode of illness.
To prevent bottlenecks, discharge planning must begin at the time of patient admission to optimize healthcare resource utilization. When patients eventually transfer units or leave the hospital, continuity of care ensures a seamless transition of patient management between different healthcare settings.
Information transfer during these transitions is highly vulnerable to error. Therefore, a standardized handoff communication tool reduces information loss during the transfer of patient care.
- Fact: SBAR is a standardized communication tool standing for Situation, Background, Assessment, and Recommendation.
At the bedside, time is your most inelastic resource. You cannot borrow it; you can only allocate it. Time management in nursing requires completing high-priority interventions before lower-priority tasks.
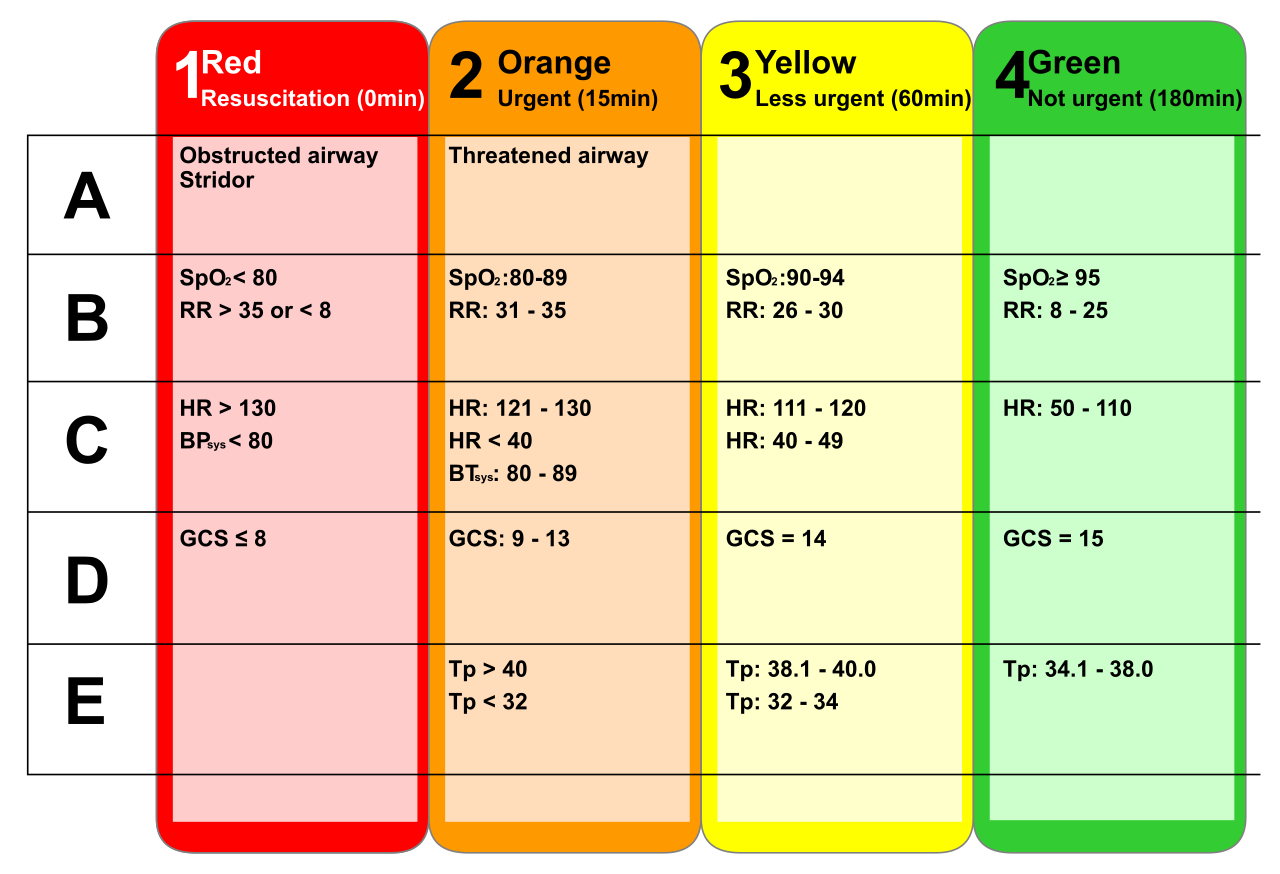
How do we sort the signal from the noise? We use an absolute hierarchy of triage:
- First-order prioritization in nursing addresses immediate life-threatening conditions (Airway, Breathing, Circulation).
- Second-order prioritization in nursing addresses urgent issues like acute pain or abnormal laboratory values (e.g., a potassium of 2.8 mmol/L).
- Third-order prioritization in nursing addresses long-term health needs or routine daily care tasks (e.g., ambulating a stable patient or routine hygiene).
Therefore, effective resource allocation requires prioritizing essential patient safety interventions over routine tasks.
Once tasks are prioritized, how do we execute them efficiently? Resource optimization includes grouping patient care activities to conserve nursing energy and simultaneously grouping patient care activities to minimize patient fatigue. If you must enter an isolation room to hang an antibiotic, you also assess the patient, check their lines, and provide necessary hygiene in that single visit.
You cannot do everything. To multiply your effectiveness, you must delegate. Delegation is the transfer of responsibility for the performance of a task from one individual to another.
However, there is a fundamental law of nursing leadership: You can transfer the task, but you cannot transfer the liability. The delegating nurse retains accountability for the final outcome of the delegated task.
To delegate safely, you must obey The Five Rights of Delegation:
- The right task
- The right circumstances
- The right person
- The right direction or communication
- The right supervision or evaluation
Crucial Scope of Practice Limitations: While you can delegate routine vitals or ambulation to a nursing assistant, unlicensed assistive personnel cannot perform initial nursing assessments, nor can they provide initial patient education. Assessment and initial teaching require the clinical judgment of an RN.
Physical and financial resources require the same meticulous care as human resources. A manager uses a nursing unit budget, which forecasts the financial resources required to operate the ward for a specific period.
Accountability in resource allocation means a nurse manager is answerable for the financial implications of staffing decisions. Similarly, accountability in resource allocation requires a nurse manager to justify the clinical necessity of equipment requests. You cannot just ask for ten new ventilators; you must prove the patient acuity demands them.
On the floor, organizing resources requires assigning physical equipment to areas of highest clinical priority. Furthermore, material resource management involves maintaining adequate par levels of essential clinical supplies on the unit.
A common psychological reaction to scarcity is hoarding. However, equipment hoarding by nursing units creates artificial shortages and delays care in other hospital areas. If the ICU hides five IV pumps "just in case," the Emergency Department cannot administer life-saving fluids.

To keep what we have functioning, preventive maintenance of medical equipment minimizes unexpected operational downtime. Ultimately, cost-effective care involves reducing supply waste without compromising the quality of patient outcomes.
If we engineer the perfect staffing ratios, implement pristine clinical pathways, and optimize our budgets, how do we prove it actually works?
We look at the evidence. Evidence-based staffing models incorporate nursing-sensitive indicators to evaluate staffing effectiveness. These are specific clinical outcomes that rise or fall in direct correlation with the quality and quantity of nursing care.
If staffing is inadequate or skill mix is poor, three metrics inevitably worsen:
- Pressure ulcer prevalence is a widely recognized nursing-sensitive indicator. (If nurses lack time to turn patients, skin breaks down).
- Patient fall rates are a widely recognized nursing-sensitive indicator. (If nurses cannot respond to call bells quickly, confused patients attempt to walk alone).
- Hospital-acquired infection rates are widely recognized nursing-sensitive indicators. (If understaffed nurses rush, sterile technique breaks down).
By tracking these indicators, nursing leadership proves that resources, staffing, and care coordination are not just administrative concepts—they are the very foundation of patient survival.