North Carolina Health Insurance Mandates & Continuation of Coverage
Every state health insurance market runs on two parallel rulebooks: the federal one (ACA, HIPAA, the Mental Health Parity and Addiction Equity Act) and the state one layered on top of it. For North Carolina, that state rulebook lives in General Statutes Chapter 58, and it is where the exam will test you hardest — because it is where a Texas-trained agent's intuition breaks down. A benefit that is federally guaranteed in one market can be silent at the state level in another, and a mandate that sounds absolute in casual conversation ("NC covers autism treatment") almost always has a carve-out buried in the statutory text. Your job is to know precisely where the carve-outs sit.
Before any mandate matters, you have to know whether a business even qualifies as a "small employer" under North Carolina law — because small-group rules (community rating, guaranteed issue, limited underwriting) only attach once that threshold is met.
Defining the Small Employer
North Carolina actually runs two definitions side by side, because the market itself is split between legacy business and post-ACA business:
Grandfathered small employer (G.S. 58-50-110): a business that employed no more than 50 eligible employees on at least 50% of its working days during the preceding calendar quarter.
Non-grandfathered small employer: averaged between 1 and 50 employees during the preceding calendar year, and employs at least 1 employee on the first day of the plan year.
Notice the different measurement windows — a calendar quarter for grandfathered groups versus a calendar year for non-grandfathered groups. An exam question that swaps these is testing whether you actually read the statute or just memorized "50 employees."
An eligible employee is defined narrowly: someone working a normal workweek of 30 or more hours. A restaurant with fifteen full-time cooks and thirty part-time servers working 20 hours a week is a small group counting only the fifteen — the part-timers don't count toward eligible-employee totals, though they may still be offered coverage under the employer's own eligibility rules.
Two anti-gaming provisions round out the definition:
- Affiliated companies that are eligible to file a combined state tax return are treated as a single employer for counting purposes. A business owner can't dodge small-group status by splitting one 80-employee company into four 20-employee shell companies.
- Group size must be redetermined annually after a plan is issued. A group that grows past 50 eligible employees doesn't stay "small" forever just because it started that way.
Rating Rules: Grandfathered vs. Non-Grandfathered
This is where the exam loves to test comparison tables, because the two regimes genuinely rate differently.
| Rating Factor | Grandfathered Small-Group | Non-Grandfathered Small-Group |
|---|---|---|
| Rating method | Adjusted community rating | Modified community rating (ACA-style) |
| Allowed rating variables | Age, gender, family size, geographic area, industry | Age, tobacco use, family size, geographic area |
| Rate variation limit | ±25% from the adjusted community rate | 3-to-1 for age (adults); 1.2-to-1 for tobacco use |
| Industry rating factor cap | — | Capped at no more than 1.2× the carrier's lowest industry rate factor |
| Rate-change lock | 12 months from issue/renewal (with limited exceptions, e.g., large membership shifts) | Same 12-month lock applies |
The intuition behind the 3-to-1 age band: without it, a carrier could charge a 63-year-old ten times what it charges a 25-year-old, effectively pricing older employees out of small-group coverage entirely. North Carolina compresses that spread to protect affordability for older workers in small businesses — the same logic that drives the 1.2-to-1 tobacco band, which limits (but doesn't eliminate) the surcharge carriers can charge smokers.
Late enrollees: North Carolina caps the combined preexisting-condition exclusion and coverage-exclusion period for late enrollees in small-group plans at a maximum of 18 months. A late enrollee isn't locked out forever — just delayed, and only up to a year and a half.
G.S. 58-3-220 is the single most commonly misunderstood mandate on this exam, because agents assume "mental health parity" means what the federal Mental Health Parity and Addiction Equity Act (MHPAEA) of 2008 means: full parity, everywhere, for everyone. North Carolina's statute is much narrower, and the narrowness is deliberate — it exists because the federal law fills the rest of the gap.
Walk through it layer by layer:
Who is covered. G.S. 58-3-220 applies only to group health benefit plans. It says nothing about individual policies.
What "mental illness" means. The statute defines mental illness by reference to DSM-5 diagnoses — but then carves three categories back out of that definition entirely:
G.S. 58-3-220 excludes autism spectrum disorder, substance-use disorders, and non-organic sexual dysfunctions from its statutory definition of "mental illness."
That matters enormously: it means the state mental-illness parity mandate has nothing to say about autism or substance-use treatment — those are governed by entirely separate statutes (autism has its own mandate, discussed below; substance-use parity comes from federal law).
How much parity is required, and for whom. Here's the layer that trips up most candidates. Full parity — the same benefit limits as physical illness, no separate visit caps — is required only for group plans covering a large employer, as defined in G.S. 58-68-25. For group plans that do not cover a large employer (i.e., small-group plans), G.S. 58-3-220 requires only minimum stated numbers of mental illness office visits and inpatient/outpatient days — not full medical-benefit parity.
And for the individual and small-group markets specifically:
North Carolina has no state statute mandating mental health parity for individual or small-group health plans. Parity in those markets comes entirely from federal law (MHPAEA operating alongside the ACA), not from North Carolina insurance statute.
Picture the full landscape as a three-tier structure:
| Market Segment | Parity Source | Standard |
|---|---|---|
| Group, large employer | G.S. 58-3-220 (state) | Full parity (same benefit limits as physical illness) |
| Group, not large employer (small-group) | G.S. 58-3-220 (state) | Minimum stated visit/day counts only |
| Individual & small-group (as a mandate source) | Federal law only | Federal MHPAEA standard, no NC statute |
The exam trap: a question describing an individual policyholder denied equal mental-health benefits and asking "which NC statute protects them" — the correct answer is that no NC statute does; the protection, if any, is federal.
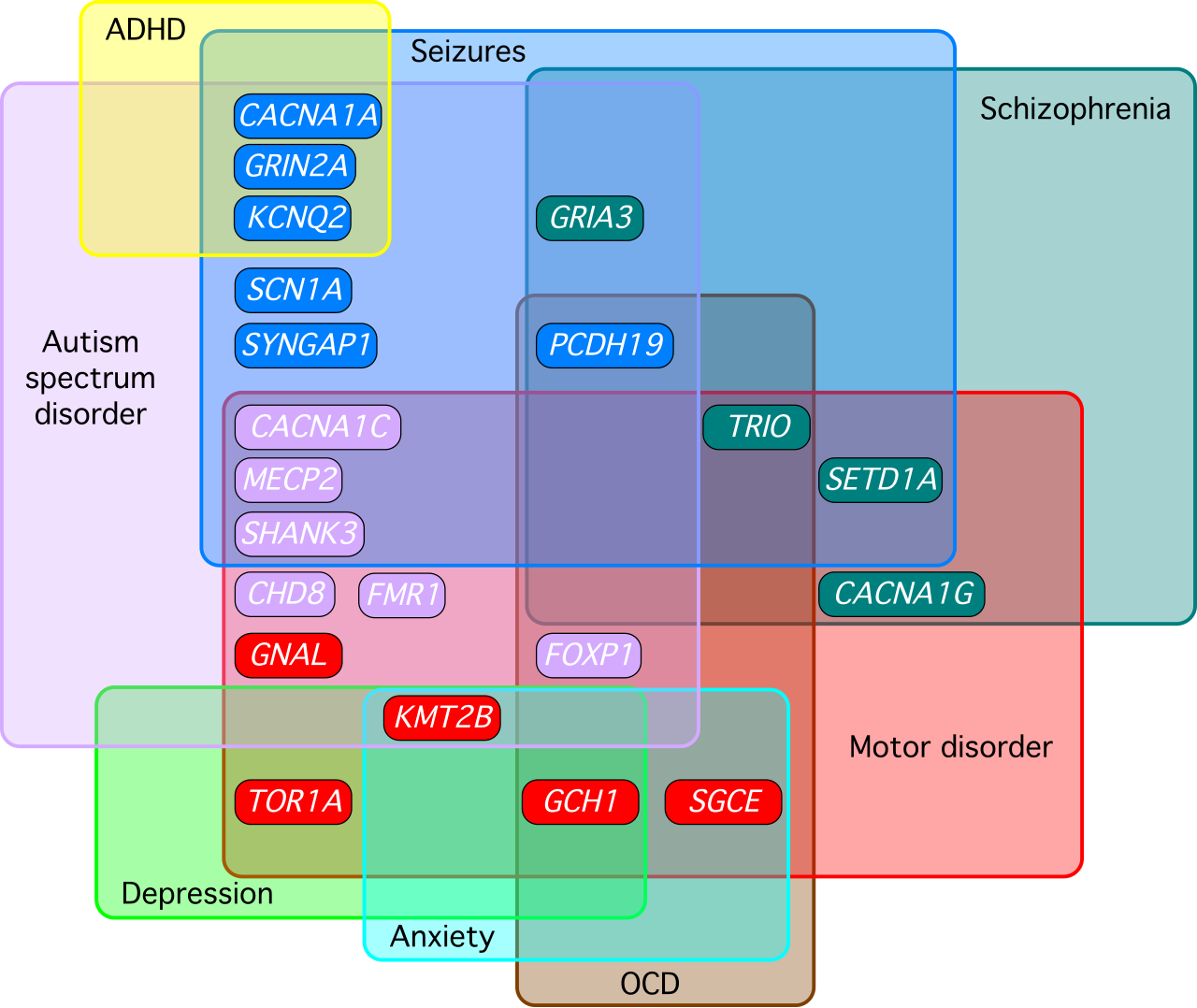
Where mental illness parity carves autism out, a separate statute carves it right back in — with its own distinct rules. G.S. 58-3-192 requires health benefit plans to cover the screening, diagnosis, and treatment of autism spectrum disorder.
The critical exam distinction is between the diagnosis mandate and the adaptive behavior treatment mandate, because they are subject to completely different limits:
No diagnosis-age cutoff. G.S. 58-3-192 does not limit its screening, diagnosis, and treatment mandate to individuals diagnosed before any specific age. A 40-year-old newly diagnosed with autism is still covered for screening and diagnosis under this statute.
Adaptive behavior treatment is different. Coverage for adaptive behavior treatment specifically is capped at $40,000 per year, and insurers are permitted (not required) to limit that particular treatment category to individuals age 18 and younger.
So two separate limits apply to two separate things: a dollar cap on adaptive behavior treatment (regardless of age), and an optional age ceiling that only touches adaptive behavior treatment — not diagnosis, not pharmacy care, not psychiatric or psychological care, not general therapeutic care. If an exam question says "NC caps autism coverage at age 23" or implies the entire mandate stops at 18, that's the myth this section exists to correct.

Finally, an anti-discrimination backstop: North Carolina prohibits insurers from terminating, refusing to issue, or refusing to renew coverage solely because an individual has an autism spectrum disorder diagnosis. The diagnosis itself can never be used as a reason to push someone out of the risk pool.
Beyond mental illness and autism, North Carolina requires several other specific benefits. Think of these as facts you should be able to recall cold, because exam questions on mandated benefits tend to be direct recall rather than scenario analysis.
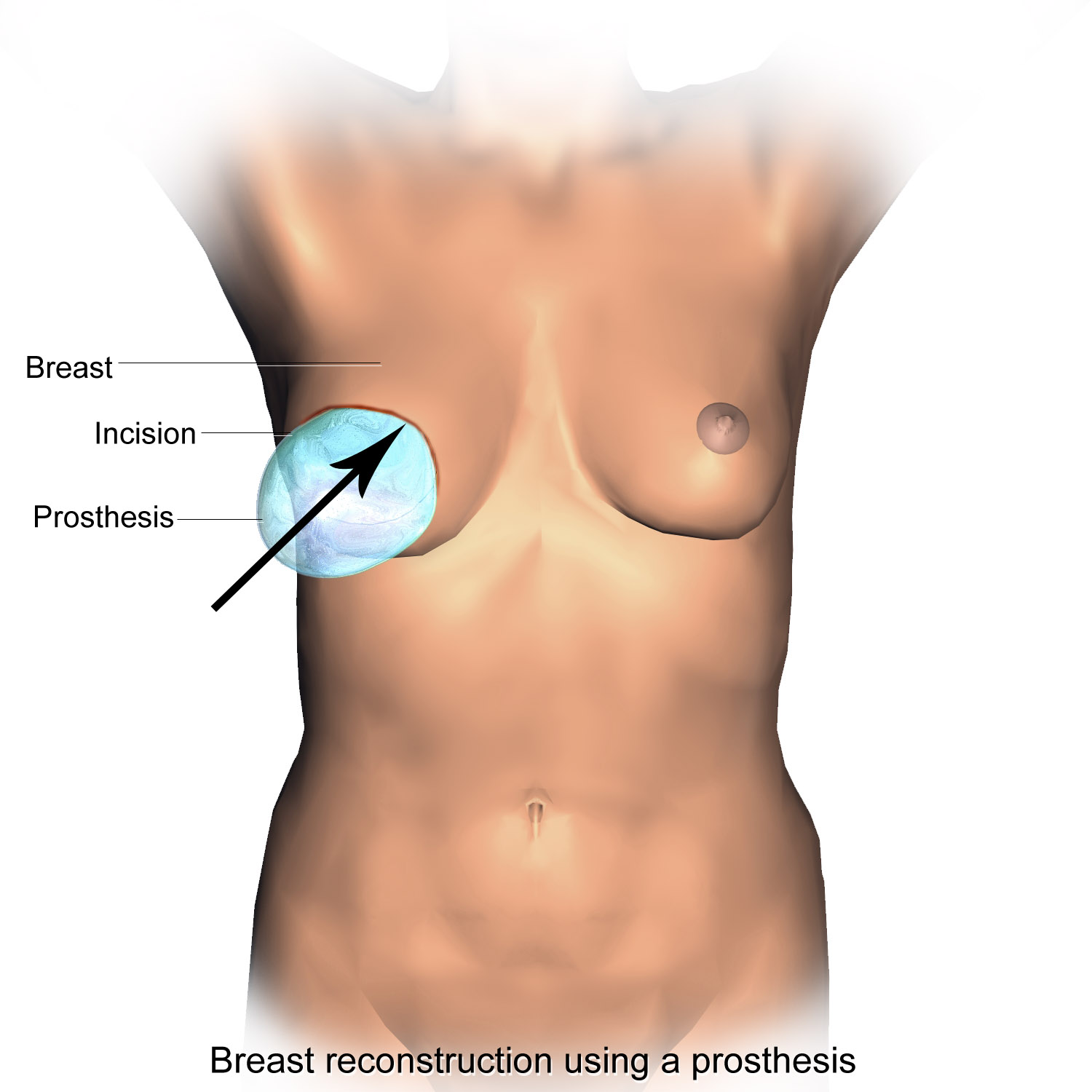
Mastectomy Reconstruction
North Carolina mandates coverage for reconstructive breast surgery following a mastectomy — and "reconstruction" is defined broadly: all stages of the reconstructive surgery, surgery on the other breast to achieve symmetry, and prostheses. A carrier can't cover only the mastectomy itself and treat reconstruction as elective cosmetic work.
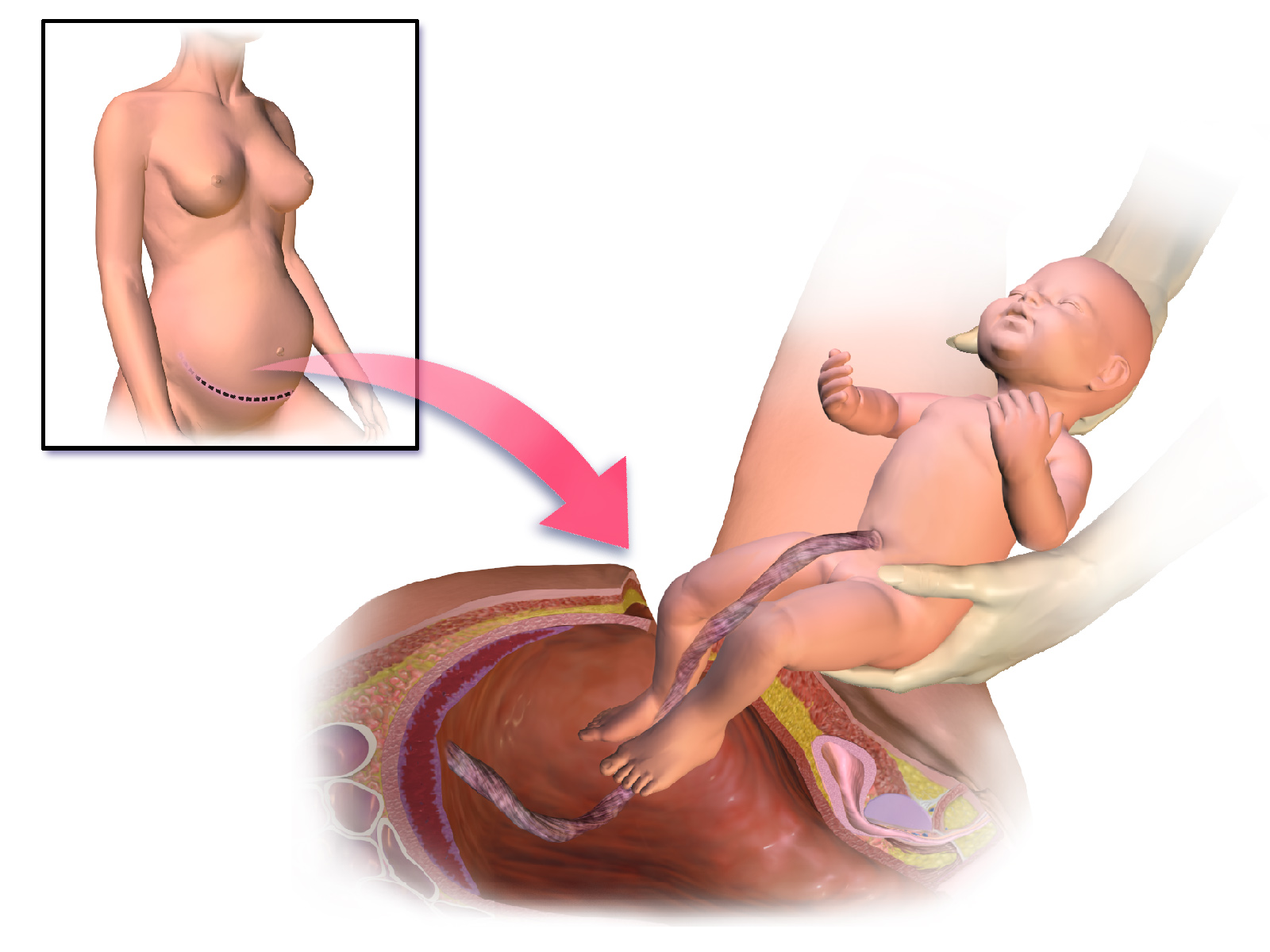
Maternity Length-of-Stay
Minimum inpatient hospital stay after a normal vaginal delivery: 48 hours. Minimum inpatient hospital stay after a cesarean section: 96 hours.
If the mother and newborn are discharged earlier than these minimums (by mutual agreement with the attending provider), the plan must still cover timely postdelivery follow-up care — the mandate doesn't disappear just because the family chose an early discharge; it converts into a follow-up-care obligation.
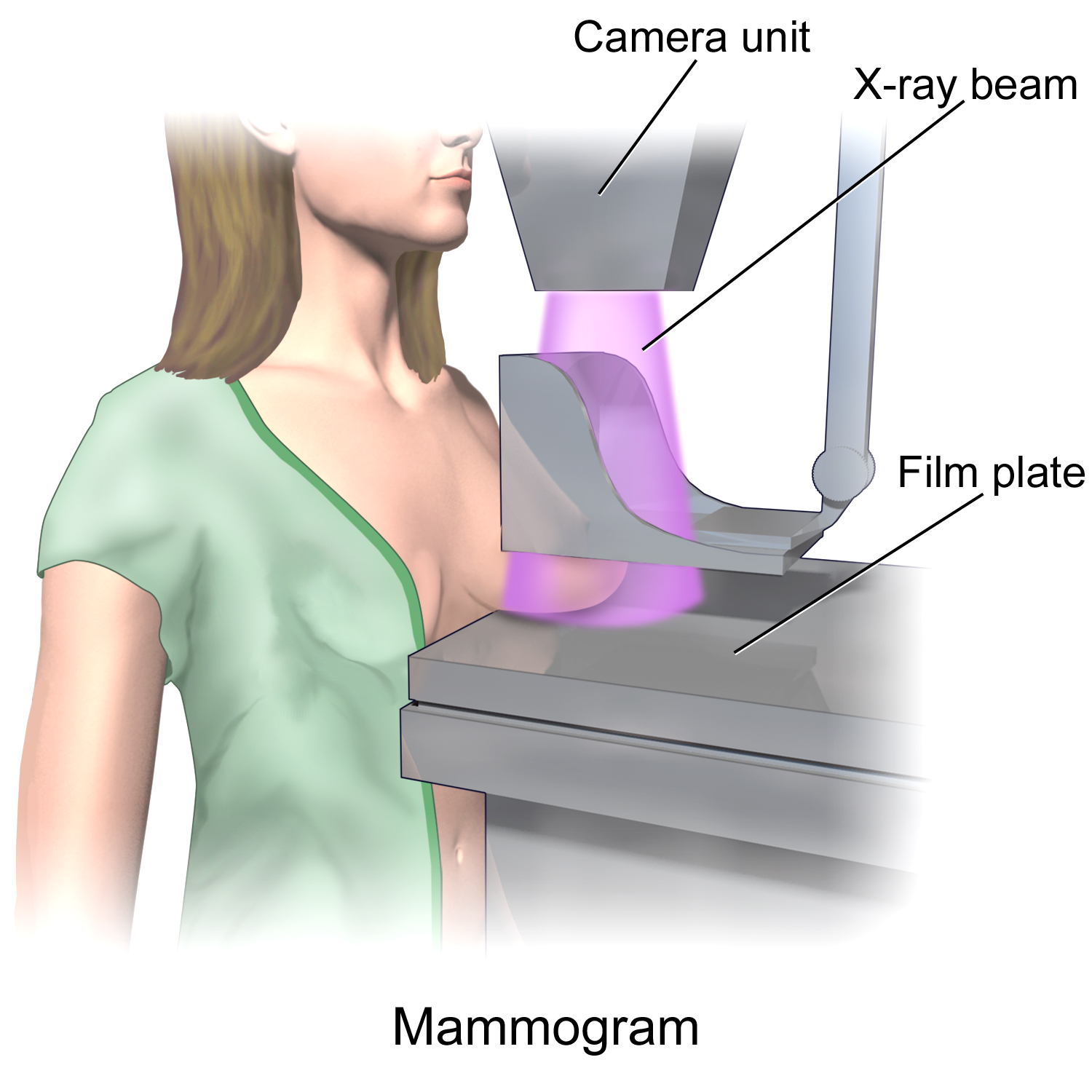
Mammography Screening — Recently Recodified
This statute moved addresses recently, and the exam may test either citation, so know both:
North Carolina's mammography screening mandate was recodified from G.S. 58-51-57 to G.S. 58-3-271, effective October 1, 2025.
The substantive schedule itself is a graduated, age-banded structure — memorize it as a ladder:
| Age Group | Required Coverage |
|---|---|
| 35–39 | One baseline low-dose screening mammogram |
| 40–49 (not elevated risk) | Low-dose screening mammogram every other year (biennial) |
| 50 and older | Annual low-dose screening mammogram |
| Any age, elevated risk (e.g., personal or close family history of breast cancer) | Annual low-dose screening mammogram |
The logic mirrors clinical screening guidelines: risk climbs with age, so frequency climbs with age, and anyone with an elevated personal risk profile jumps straight to the annual tier regardless of where they'd otherwise fall on the age ladder.
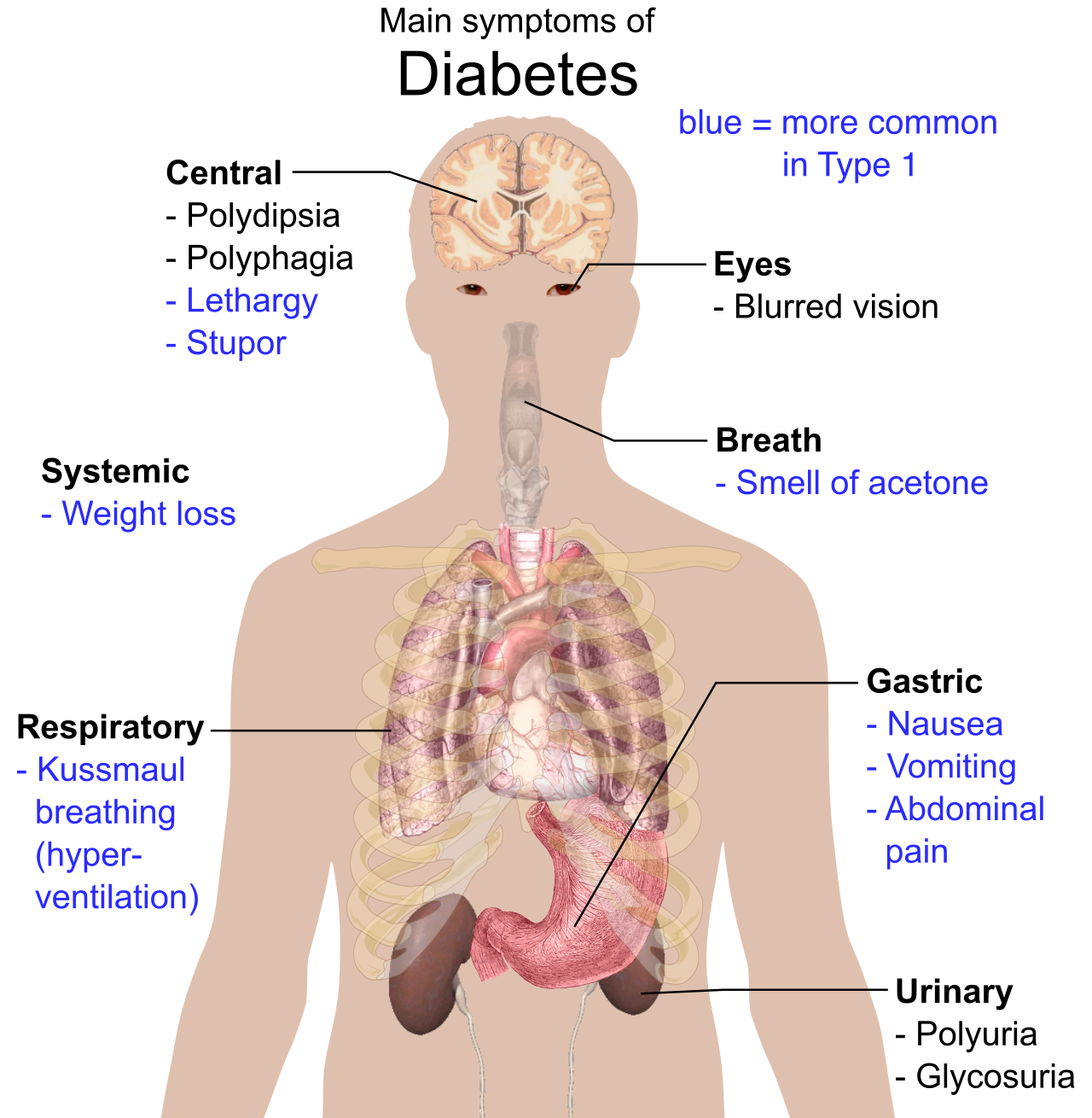
Diabetes Management
North Carolina mandates coverage for diabetes outpatient self-management training, educational services, equipment, supplies, and medications. Critically, this coverage must carry the same deductibles, coinsurance, and limitations that apply to other similar medical services under the same policy — a carrier cannot single out diabetes supplies for a higher cost-sharing tier just because the mandate compels coverage.
Newborn, Adopted, and Foster Child Coverage
A newborn is covered from the moment of birth, with no requirement that the parent notify the insurer first — the coverage attaches automatically. However:

If an additional premium is required to continue covering the newborn beyond the birth event, the child must be enrolled within 30 days of birth for that continued coverage to take effect.
Foster children and adopted children receive the identical treatment as newborns — coverage attaches upon placement in the home (foster) or placement for adoption, with the same automatic-eligibility logic.
One more protection worth flagging: North Carolina prohibits individual health insurers from imposing a preexisting-condition exclusion on a newborn who has creditable coverage as of the 30th day after birth. A family that keeps the newborn continuously covered from birth can't later be hit with a preexisting-condition denial in the individual market.
Grace Period (Standard Provision)
North Carolina's standard accident and health policy grace-period provision sets minimums by premium mode:
| Premium Payment Mode | Minimum Grace Period |
|---|---|
| Weekly | 7 days |
| Monthly | 10 days |
| All other modes | 31 days |
Medigap is federally standardized by plan letter (A through N), but North Carolina layers state-specific consumer protections on top, and the Department of Insurance regulates the plans sold in-state.

Open Enrollment
North Carolina's Medicare supplement open enrollment period begins the first month a person is both age 65 or older and enrolled in Medicare Part B. It lasts six months and is a one-time, non-recurring window.
During this six-month window, an insurer must issue any Medigap plan it sells, regardless of medical condition, claims experience, or health status — this is the guaranteed-issue engine that protects newly Medicare-eligible seniors from being medically underwritten out of coverage.
Guaranteed Issue for the Under-65 Disabled
Historically, many states let insurers restrict Medigap sales to age-65-and-older applicants, leaving younger Medicare beneficiaries (those who qualify through disability) without a guaranteed path to supplemental coverage. North Carolina closed that gap:
G.S. 58-54-45, effective January 1, 2020, guarantees individuals under age 65 who qualify for Medicare due to disability the right to purchase Medigap Plan A, D, or G.
The Plan-Letter Cutover: Pre-2020 vs. Post-2020 Eligibility
This is a frequently tested wrinkle, because the plans offered to a new Medigap applicant depend on when their Medicare eligibility began — not on when they're shopping today.
| Medicare Eligibility Began | Plans That May Be Offered |
|---|---|
| Before January 1, 2020 | A, C, or F |
| On or after January 1, 2020 | A, D, or G (in place of C and F) |
The reason: federal law phased out sales of Plans C and F (the plans covering the Part B deductible) to anyone newly eligible for Medicare on or after that date, to reduce first-dollar coverage incentives for overutilization. North Carolina's offering structure simply mirrors that federal cutover.
Additional Guaranteed-Issue Trigger: Managed Care Disenrollment
A Medicare beneficiary disenrolled from a managed care plan (e.g., a Medicare Advantage plan) gets a guaranteed-issue right to buy Medigap Plan A, D, or G from any insurer, as long as they act within 63 days of termination or disenrollment.
Core Consumer Protections
- 30-day free-look period, with premium refunds paid directly to the applicant.
- No duplication of Medicare benefits — a Medigap policy cannot contain benefits that simply repeat what Medicare already pays.
- Guaranteed renewable as long as the required premium is paid.
- Outline of coverage required, describing principal benefits, exceptions, reductions, limitations, and renewal provisions — so the applicant can compare plans on an apples-to-apples basis before buying.
Federal COBRA only applies to employer groups with 20 or more employees. Every producer in North Carolina will eventually place a client at a 12-person business whose group coverage just terminated — and for that client, federal COBRA doesn't exist. This is exactly the gap North Carolina's own continuation law fills.
G.S. Chapter 58, Article 53 gives an employee or member the right to continue group hospital, surgical, and major medical coverage after employment or membership terminates. It functions as a "mini-COBRA," commonly relied on by employer groups too small to be subject to federal COBRA.

Memorize the mechanics as a single sequence — it's tested as a checklist:
| Requirement | Standard |
|---|---|
| Prior continuous coverage required | 3 consecutive months immediately before termination |
| Election window | At least 60 days after termination or loss of eligibility |
| Maximum continuation period | 18 months after coverage would otherwise have ended |
| Premium cap | 102% of the full group rate |
| Benefits included | Hospital, surgical, major medical only — dental, vision, and prescription drug benefits are not required |
Two nuances the exam likes to probe: first, the 102% cap means the continuee can be charged a small administrative markup over the group rate — not the group rate exactly, and not an unlimited "COBRA-style" markup either. Second, the benefit scope is narrower than many candidates assume — a continuee keeps their major medical protection, but a standalone dental or vision rider does not automatically continue with it.
Conversion: What Happens After the 18 Months (or Instead of Continuation)
When group coverage ends and the person wants to move to an individual policy rather than (or after) continuing group coverage:
Written application and the first premium payment for an individual conversion policy must reach the insurer no later than 31 days after group coverage terminates. The conversion policy must be issued without evidence of insurability — the insurer cannot medically underwrite the applicant or deny the conversion based on health status.
How State Continuation Ends
Coverage under state continuation terminates at the earliest of:
- The 18-month maximum being reached,
- Nonpayment of the required premium,
- The continuee becoming eligible for other group coverage, or
- Termination of the underlying group policy itself.
Think of these four triggers as an "OR" gate — any single one of them cuts the continuation off immediately, regardless of how much of the 18 months remains.
Every rule in this topic traces back to the same underlying tension: North Carolina's insurance code exists to keep coverage attainable for people at their most vulnerable moments — losing a job, having a baby, aging into Medicare, receiving an autism diagnosis — while still leaving carriers a viable, actuarially sound market to sell into. The mandates are specific, the percentages and day-counts are exact, and the exam rewards candidates who can state the precise number rather than the general idea. When in doubt, anchor to the statute number and the exact figure: 3-to-1, 1.2-to-1, 102%, 18 months, 60 days, 31 days, $40,000, 30 days, 63 days — these are the load-bearing numbers of the entire topic.