Critical Care Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Managing a critically ill patient is a real-time exercise in applied physics, fluid dynamics, and electrophysiology, executed under the highest possible stakes. When you are standing at the bedside of a patient in septic shock or multiorgan failure, you are not merely executing tasks; you are acting as the conductor of a highly complex physiological orchestra. In the Saudi Intensive Care Unit, this physiological mastery must be seamlessly combined with stringent infection control protocols and deeply rooted ethical frameworks.
To excel on the Saudi Nursing Licensure Examination (SNLE), you must stop memorizing disconnected facts and start visualizing the body as a continuous mechanical system. Let us deconstruct the architecture of critical care nursing.
Human life relies on the uninterrupted delivery of oxygenated blood to the tissues. The cardiovascular system achieves this through an elegant relationship between a pump (the heart), the pipes (the vasculature), and the fluid within (blood).
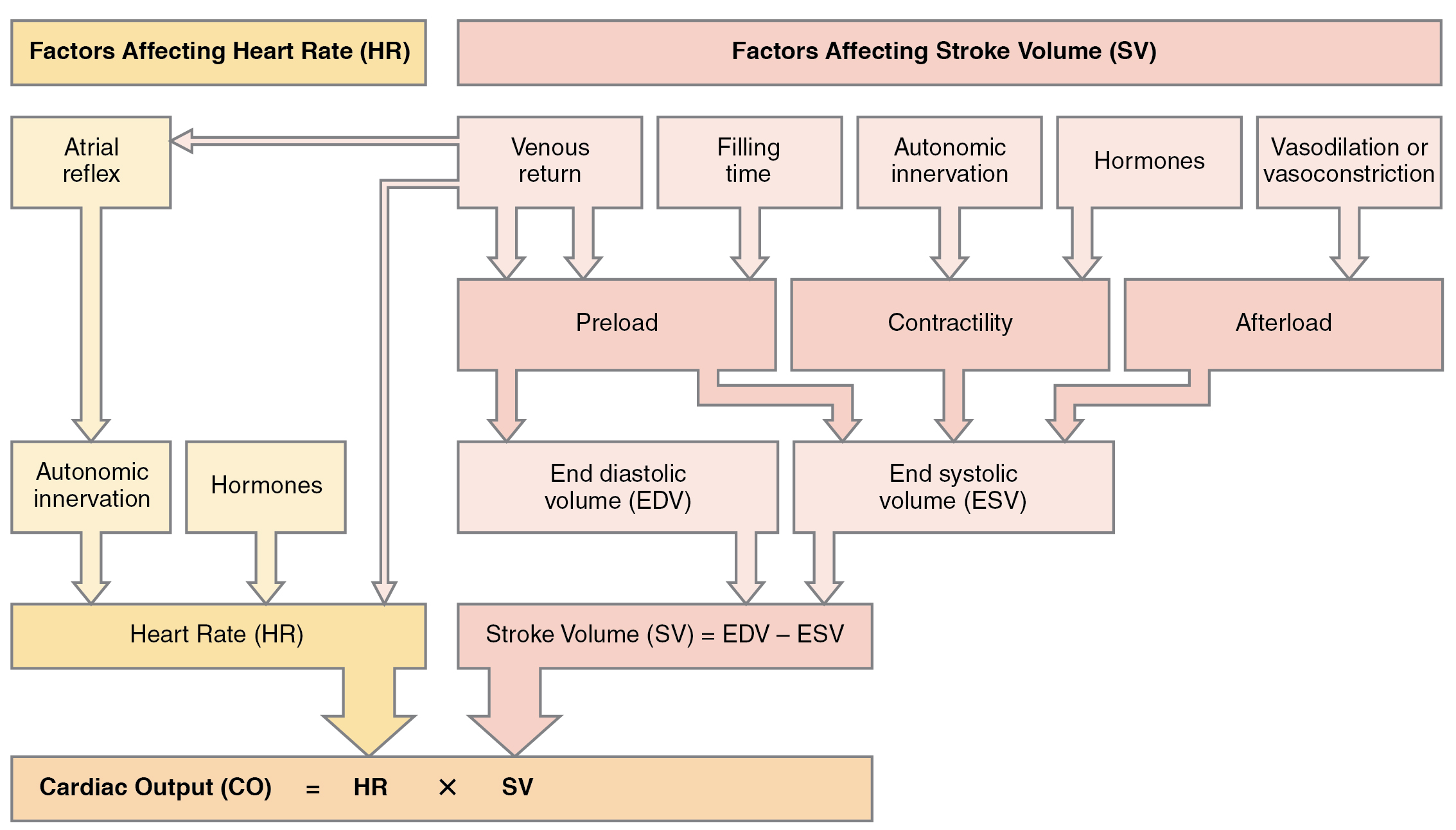
Cardiac output—the total volume of blood the heart pumps in one minute—is calculated by multiplying heart rate by stroke volume.
- Normal resting cardiac output ranges from 4 to 8 liters per minute.
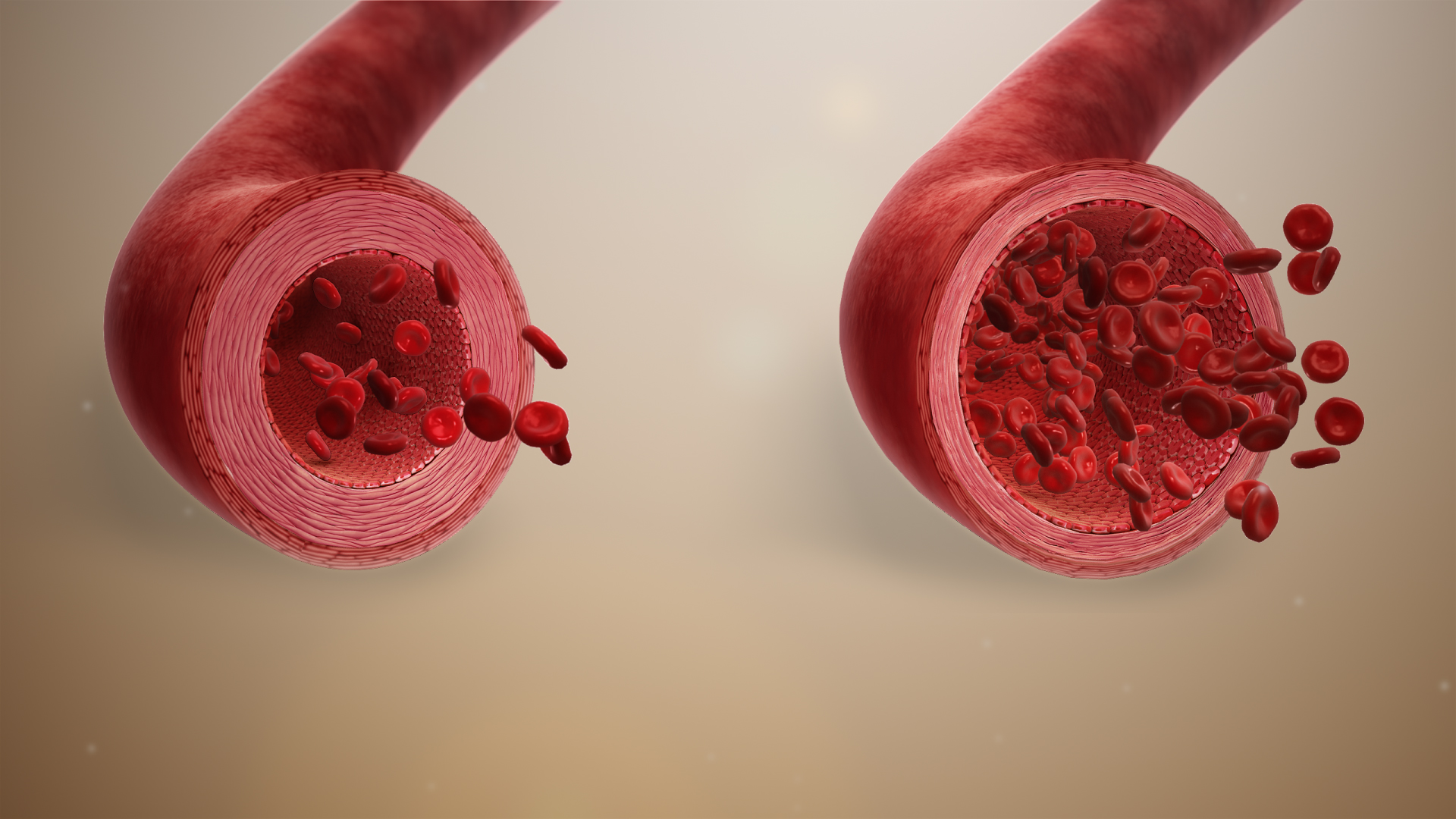
The resistance that this blood meets as it travels through the peripheral arteries is the systemic vascular resistance (SVR).
- The normal range for systemic vascular resistance (SVR) is 800 to 1200 dynes/sec/cm^-5.
When a patient develops distributive shock, such as sepsis, bacterial endotoxins paralyze the smooth muscle in the blood vessels. The pipes dilate massively. Because of this vasodilation, systemic vascular resistance (SVR) is significantly decreased in distributive shock states such as sepsis.
Mean Arterial Pressure (MAP) and Vasopressors
To understand if your patient's organs are actually receiving that blood, we look at the Mean Arterial Pressure (MAP).
Formula: MAP = [Systolic Blood Pressure + 2(Diastolic Blood Pressure)] ÷ 3
Why twice the diastolic? Because the heart spends roughly two-thirds of its cardiac cycle resting and filling (diastole).
- Normal mean arterial pressure (MAP) ranges from 70 to 105 mmHg.
- In the ICU, Mean arterial pressure (MAP) must be maintained at or above 65 mmHg to ensure adequate tissue perfusion in septic shock.
If the patient's MAP drops below 65 mmHg despite intravenous fluids, the pipes need to be tightened. Norepinephrine is the first-line vasopressor for the treatment of septic shock because of its profound alpha-1 adrenergic agonism, which powerfully constricts the peripheral vasculature.
Venous and Arterial Monitoring
To accurately monitor volume status, we measure Central Venous Pressure (CVP) through a central line sitting just outside the right atrium.
- Normal Central Venous Pressure (CVP) ranges from 2 to 8 mmHg.
- Think of CVP as the tank indicator. A Central Venous Pressure (CVP) reading below 2 mmHg typically indicates hypovolemia (the tank is empty).
- Conversely, a Central Venous Pressure (CVP) reading above 8 mmHg indicates hypervolemia or right-sided heart failure (blood is backing up into the venous system).
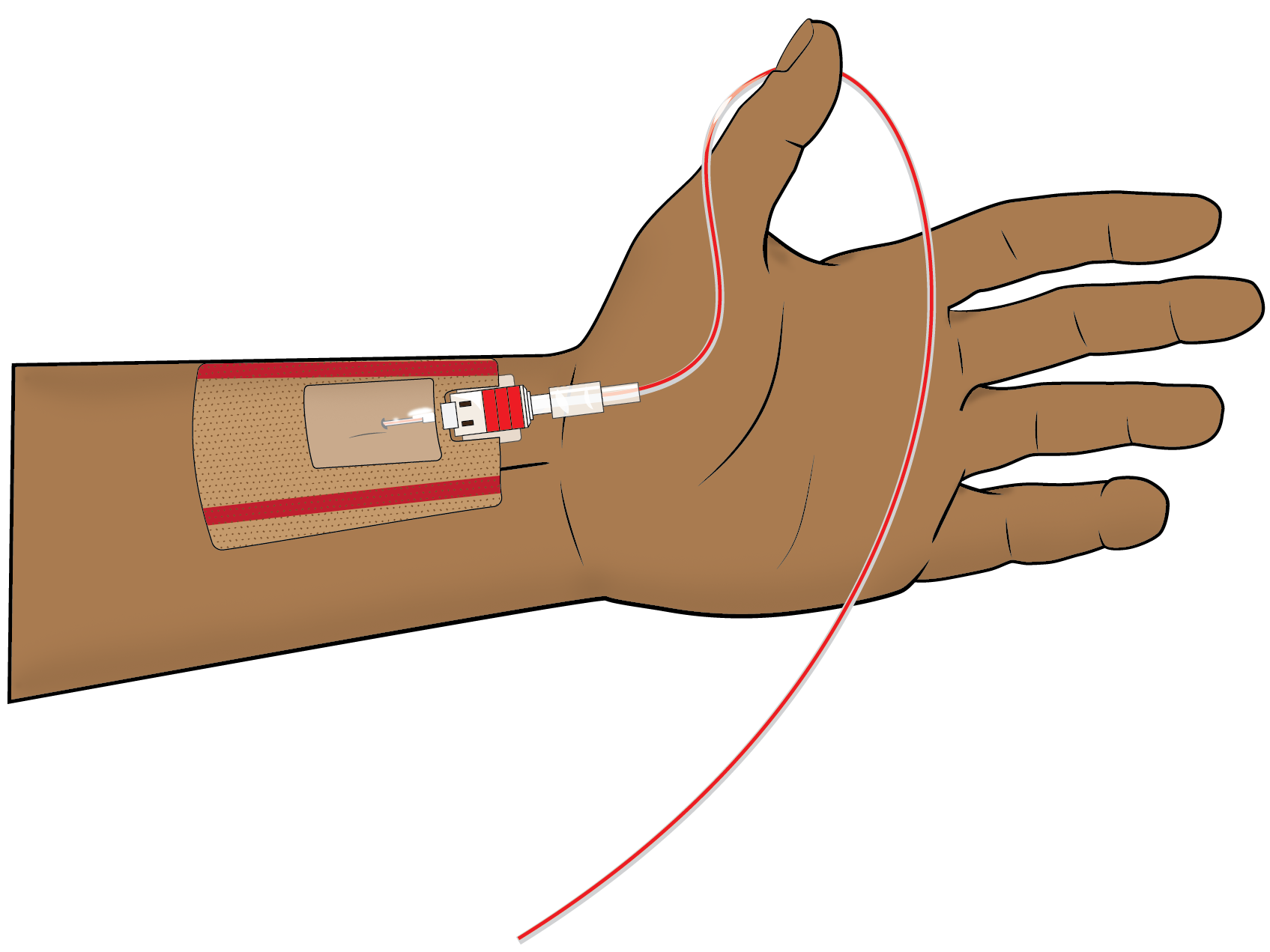
To monitor systemic blood pressure continuously, we use invasive arterial lines. For the monitor to accurately translate fluid pressure into electrical data, we must account for gravity. We do this by zeroing and leveling the system to the phlebostatic axis, which is structurally located at the intersection of the fourth intercostal space and the midaxillary line (approximating the level of the right atrium).
Leveling an arterial line transducer to the phlebostatic axis ensures accurate invasive blood pressure readings.
- An arterial line transducer placed lower than the phlebostatic axis will produce falsely high blood pressure readings because gravity adds hydrostatic pressure to the fluid column.
- An arterial line transducer placed higher than the phlebostatic axis will produce falsely low blood pressure readings because gravity pulls fluid away from the sensor.
Critical care nursing requires absolute fluency in acid-base balance. You must recognize when the lungs fail to excrete carbon dioxide.
- The normal range for arterial blood pH is 7.35 to 7.45.
- The normal range for arterial partial pressure of carbon dioxide (PaCO2) is 35 to 45 mmHg.
- The normal range for arterial bicarbonate (HCO3) is 22 to 26 mEq/L.
When ventilation fails, CO2 accumulates, converting into carbonic acid in the blood. Thus, respiratory acidosis is characterized by an arterial blood pH below 7.35 and a PaCO2 above 45 mmHg.
Mechanical Ventilation: PEEP and Pressures
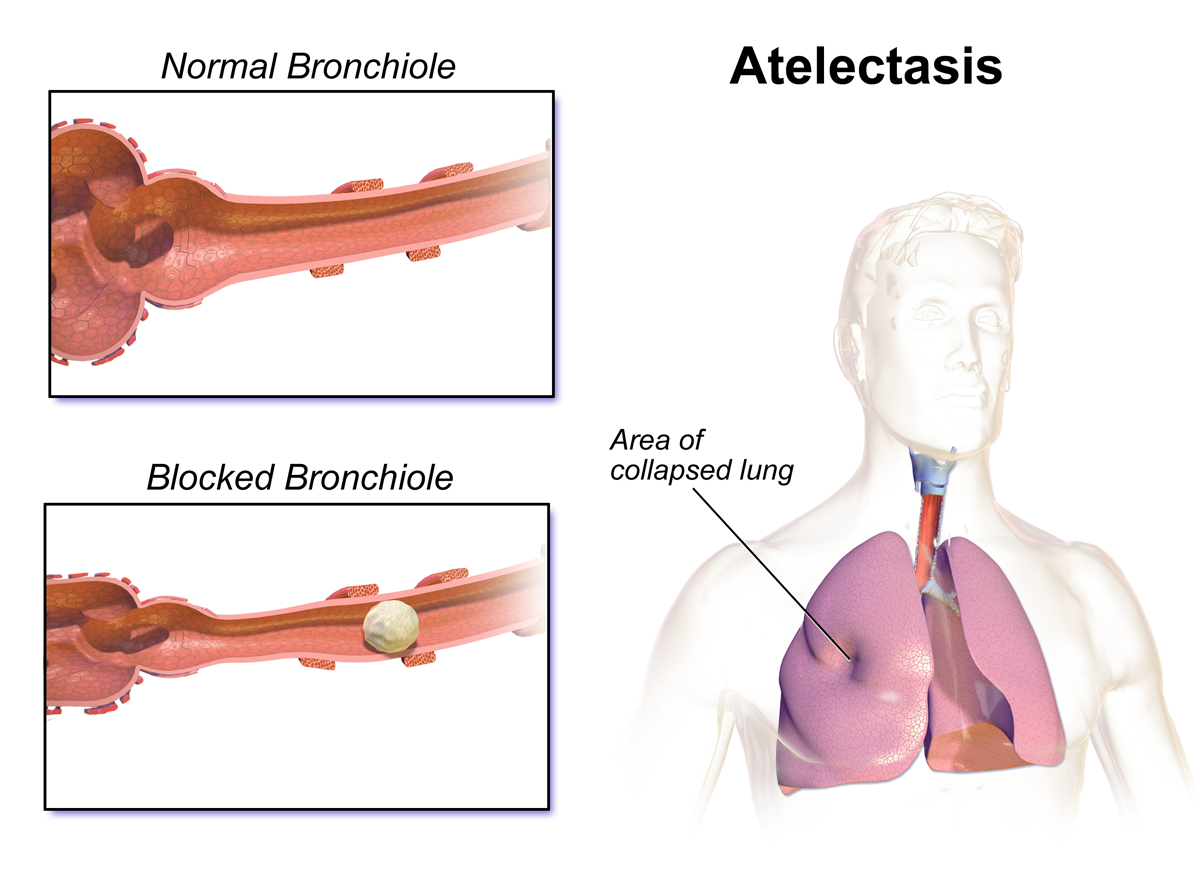
When a patient is intubated, we use Positive End-Expiratory Pressure (PEEP), which prevents alveolar collapse during expiration in mechanically ventilated patients. However, pushing continuous pressure into the closed box of the chest cavity comes with a severe hemodynamic cost.
High levels of Positive End-Expiratory Pressure (PEEP) can decrease venous return to the heart because the expanded lungs physically compress the superior and inferior vena cava. Ultimately, this decreased venous return resulting from high Positive End-Expiratory Pressure (PEEP) causes a reduction in cardiac output.
Managing ARDS
This dynamic becomes paramount when treating Acute Respiratory Distress Syndrome (ARDS). This condition represents massive inflammatory damage to the alveolar-capillary membrane.
- Clinically, Acute Respiratory Distress Syndrome (ARDS) presents with bilateral pulmonary infiltrates on a chest X-ray (often described as "white-out" lungs).
- Because the lungs become stiff and non-compliant, Acute Respiratory Distress Syndrome (ARDS) requires low tidal volume ventilation to prevent barotrauma (rupturing the fragile alveoli).
Decoding Ventilator Alarms
Mechanisms fail for entirely physical reasons. Understand the alarms:
| Alarm Type | Underlying Physics | Common Causes |
|---|---|---|
| High-Pressure | High-pressure ventilator alarms trigger when the machine encounters excessive airway resistance to delivering the set tidal volume. The air is hitting a physical roadblock. | Accumulated secretions in the patient airway cause high-pressure ventilator alarms. Furthermore, a patient biting the endotracheal tube causes a high-pressure ventilator alarm. |
| Low-Pressure | Air is escaping into the room rather than entering the lungs. The circuit lacks expected resistance. | Low-pressure ventilator alarms trigger when the mechanical ventilator circuit becomes disconnected. Alternatively, a deflated endotracheal tube cuff leak triggers a low-pressure ventilator alarm. |
The Pleural Space and Chest Tubes
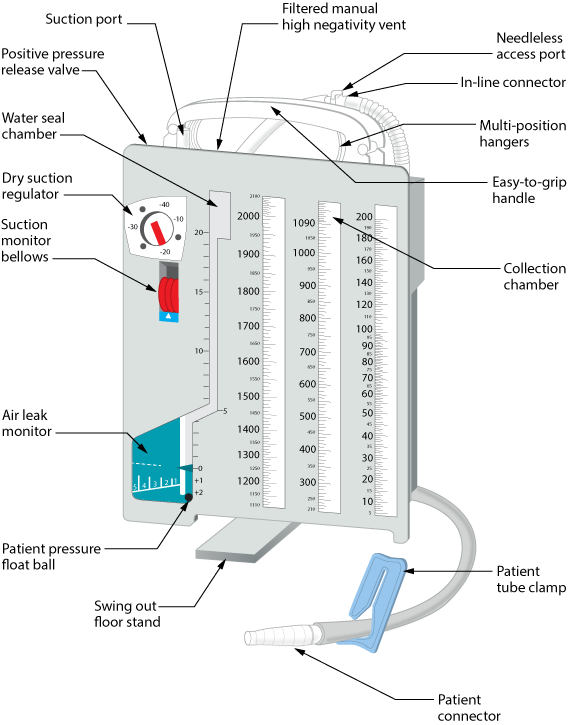
When the pleural space is violated by a pneumothorax or hemothorax, we insert a chest drain to restore negative pressure. The water-seal chamber acts as a one-way valve, letting air out but not back in.
- Tidaling in the water-seal chamber of a chest drain indicates a patent and functioning chest tube system. The water level rises and falls with inspiration and expiration.
- Intermittent bubbling in the water-seal chamber of a chest drain is a normal finding during exhalation for a patient with a pneumothorax as the trapped air is expelled.
- However, continuous bubbling in the water-seal chamber of a chest drain indicates an active air leak in the system, meaning room air is entering the circuit.
- Crucially, clamping a chest tube is contraindicated except when changing the drainage system or assessing the source of an air leak, as clamping can rapidly precipitate a deadly tension pneumothorax.
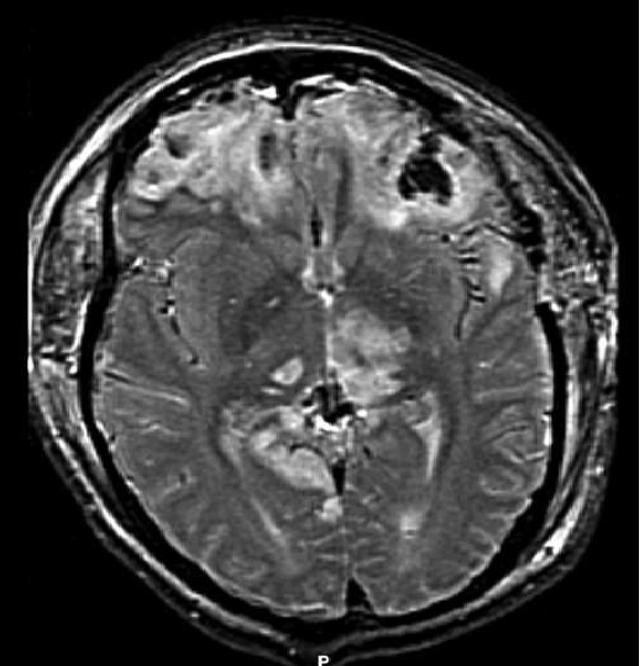
The skull is a rigid, bony box containing three components: brain tissue, blood, and cerebrospinal fluid (CSF). An increase in the volume of any one component must result in the displacement of another, or pressure will rise.
- Normal Intracranial Pressure (ICP) ranges from 5 to 15 mmHg.
- Intracranial Pressure (ICP) sustained above 20 mmHg requires immediate medical intervention to prevent brain damage.
To know if the brain is actually receiving blood, we calculate the Cerebral Perfusion Pressure (CPP).
Formula: Cerebral Perfusion Pressure (CPP) is calculated by subtracting Intracranial Pressure (ICP) from Mean Arterial Pressure (MAP). (CPP = MAP - ICP).
If ICP is too high, it physically opposes the MAP trying to push blood into the head. The target Cerebral Perfusion Pressure (CPP) for severe traumatic brain injury is 60 to 70 mmHg.
Neurological Assessment and Interventions
Neurological decline is measured via the Glasgow Coma Scale (GCS), which assesses eye opening, verbal response, and motor response. A rapid decline requires decisive action: a Glasgow Coma Scale (GCS) score of 8 or less indicates severe head injury and typically necessitates endotracheal intubation ("Less than eight, intubate").
To lower dangerously high ICP, we use basic physics:
- Gravity: Elevating the head of the bed to 30 degrees promotes cerebral venous drainage. By allowing blood to fall back to the heart, promoting cerebral venous drainage directly decreases Intracranial Pressure (ICP).
- Chemistry (Vasoconstriction): As a temporary rescue maneuver, therapeutic hyperventilation lowers arterial PaCO2 to induce cerebral vasoconstriction. When blood vessels in the brain shrink, there is less blood volume in the skull. Thus, the induced cerebral vasoconstriction from hyperventilation transiently decreases Intracranial Pressure (ICP).
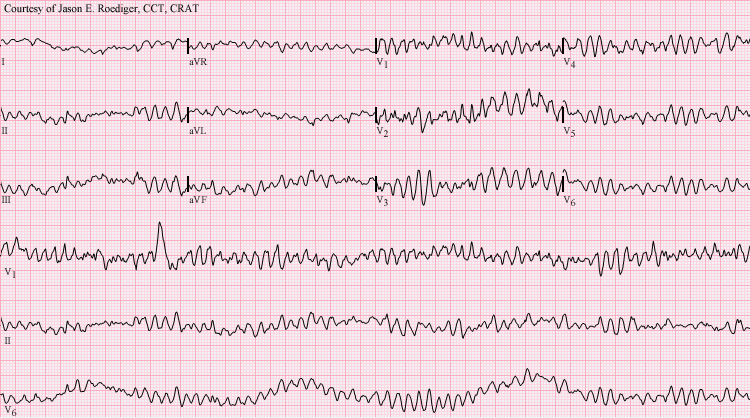
When the electrical conduction of the heart degrades, perfusion ceases. Your response hinges on identifying whether the rhythm is "shockable" (capable of being reset by electricity).
Ventricular fibrillation requires immediate high-quality cardiopulmonary resuscitation (CPR) and defibrillation. It is a chaotic, non-perfusing rhythm. If the heart refuses to stabilize, intravenous amiodarone is indicated for refractory ventricular fibrillation.
Conversely, some rhythms show electrical activity but yield no mechanical pump action.
- Pulseless electrical activity (PEA) is a non-shockable rhythm during cardiac arrest.
- Asystole is a non-shockable rhythm during cardiac arrest.
For PEA and Asystole, electricity will not work. The management of pulseless electrical activity (PEA) involves continuous cardiopulmonary resuscitation (CPR) and addressing reversible causes. During any cardiac arrest, epinephrine is administered every 3 to 5 minutes to drastically squeeze peripheral vessels and redirect blood flow to the heart and brain.
The reversible causes of cardiac arrest are commonly categorized as the 5 Hs and 5 Ts (Hypovolemia, Hypoxia, Hydrogen ion/acidosis, Hypo/Hyperkalemia, Hypothermia; Tension pneumothorax, Tamponade, Toxins, Thrombosis-pulmonary, Thrombosis-coronary). Of these, hypovolemia and hypoxia are two of the most frequent reversible causes of cardiac arrest.
Critically ill patients frequently experience acute kidney injury, losing the ability to excrete fluid and potassium.
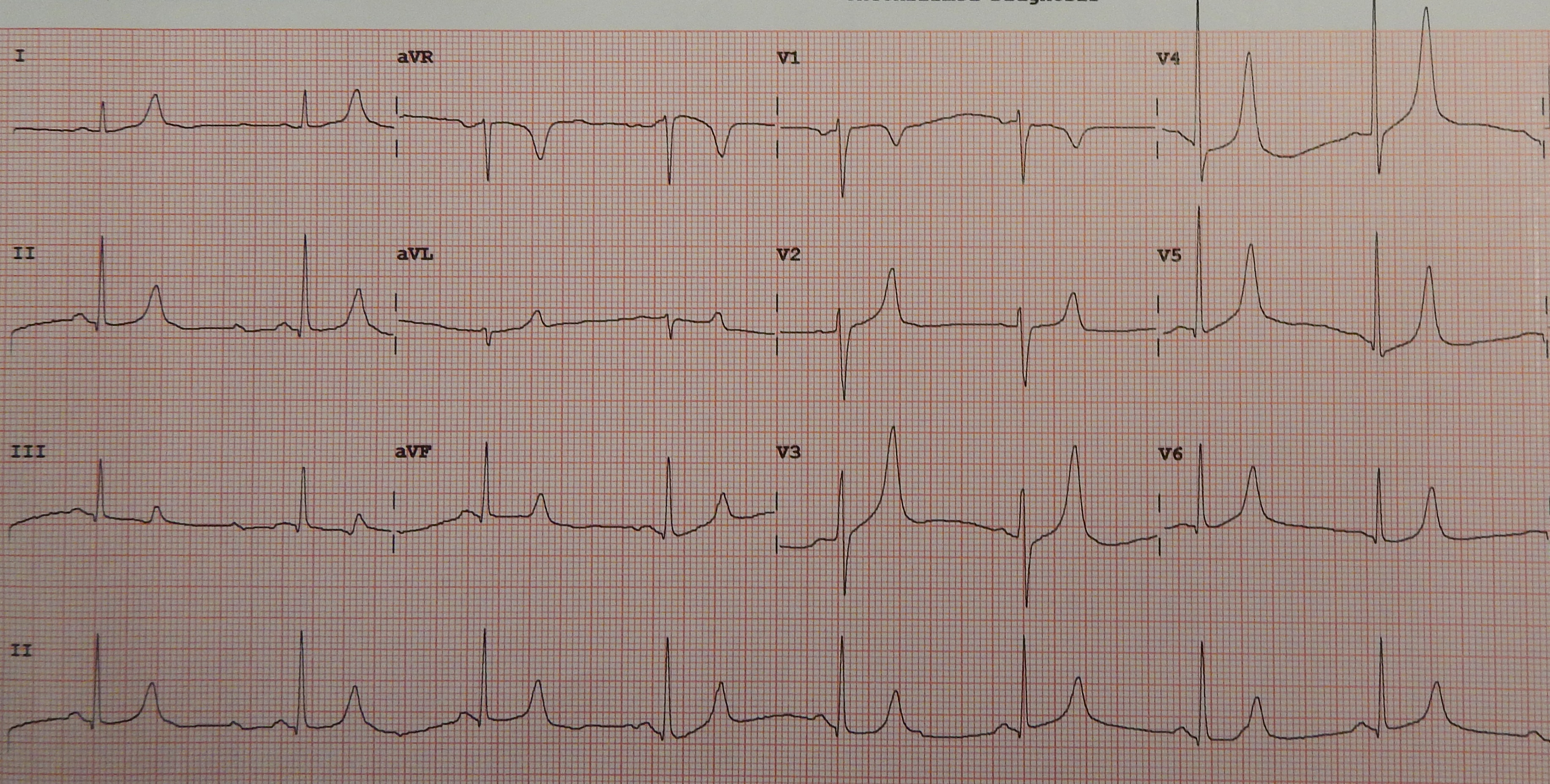
Potassium governs the repolarization of the cardiac muscle. When potassium levels rise dangerously, the electrical gradient becomes volatile. Hyperkalemia causes tall, peaked T waves on an electrocardiogram (ECG). To prevent this from degrading into a lethal arrhythmia, intravenous calcium gluconate is administered in severe hyperkalemia to stabilize the myocardial cell membrane. Note that calcium does not lower the potassium level; it acts as an immediate biological shield for the heart.
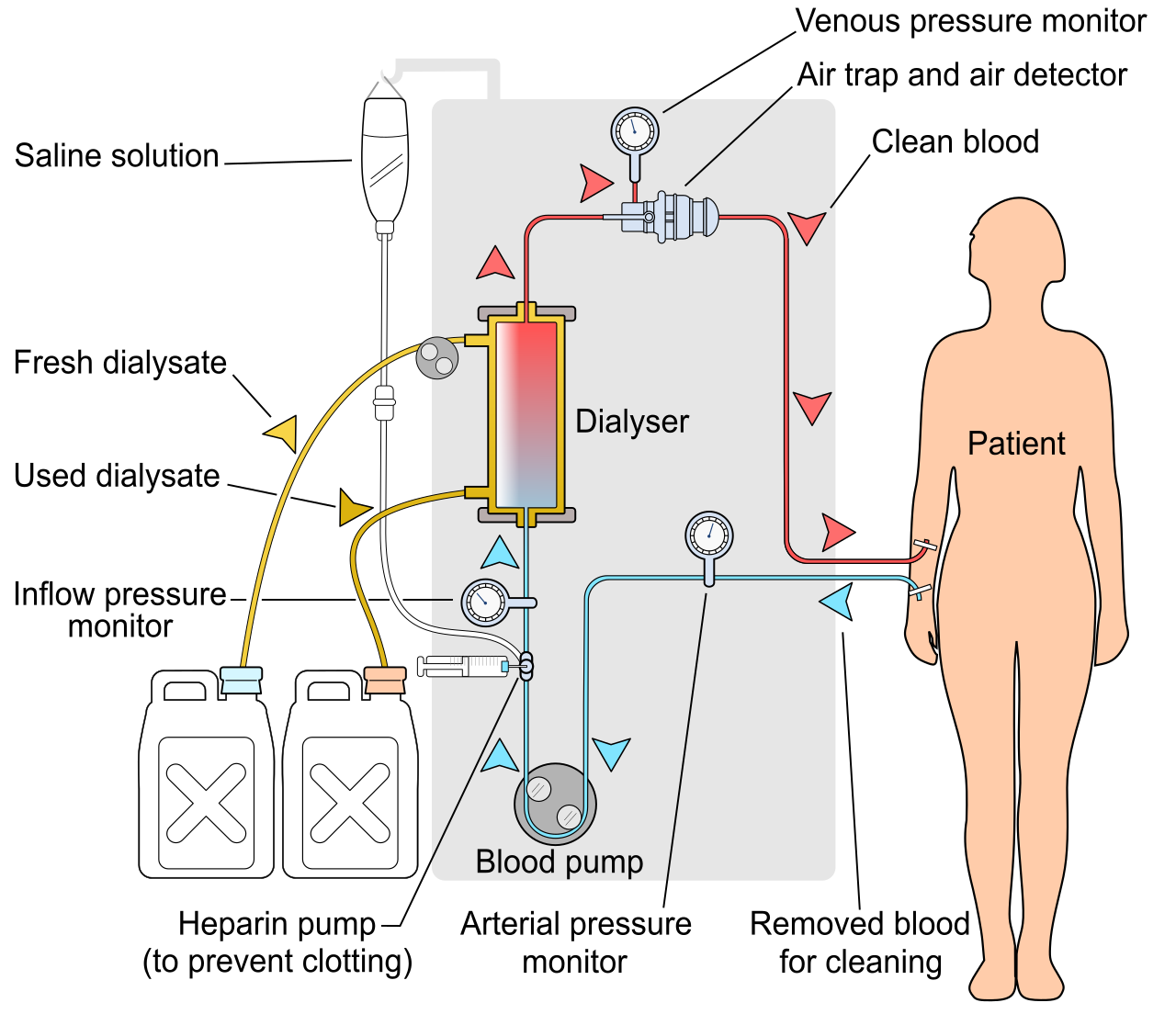
When the kidneys fail entirely in a hemodynamically unstable patient, traditional hemodialysis will crash their blood pressure. Instead, we use Continuous Renal Replacement Therapy (CRRT), which provides slow, gradual fluid removal for hemodynamically unstable patients.
Infection and delirium are quiet killers in the ICU. Strict adherence to evidence-based bundles is required for professional practice in Saudi Arabia.
Central Lines and Foley Catheters
- Central Line-Associated Bloodstream Infection (CLABSI) prevention requires maximum sterile barrier precautions during catheter insertion (cap, mask, sterile gown, sterile gloves, full-body drape).
- Once the line is in, maintenance is paramount: scrubbing the central line needleless connector hub with an antiseptic prior to access reduces the risk of Central Line-Associated Bloodstream Infection (CLABSI).
- For urinary systems, Catheter-Associated Urinary Tract Infection (CAUTI) prevention requires keeping the drainage bag continuously below the level of the patient's bladder to prevent retrograde flow of infected urine.
- Importantly, routine changing of indwelling urinary catheters is not recommended for preventing Catheter-Associated Urinary Tract Infections (CAUTI), as breaking the closed system introduces new pathogens.
The Ventilator-Associated Pneumonia (VAP) Bundle
- The Ventilator-Associated Pneumonia (VAP) prevention bundle requires elevating the head of the bed to 30 to 45 degrees to prevent micro-aspiration of gastric contents.
- Daily sedation interruptions are a core component of the Ventilator-Associated Pneumonia (VAP) prevention bundle, allowing assessment of neurological readiness to extubate.
- Furthermore, regular oral care with chlorhexidine reduces the incidence of Ventilator-Associated Pneumonia (VAP).
Sedation, Delirium, and Nutrition
Continuous sedation requires specific pharmacologic knowledge:
- Propofol is a short-acting intravenous anesthetic used for continuous sedation in mechanically ventilated patients. Because it is carried in fat, continuous propofol infusion requires routine monitoring of serum triglycerides due to its lipid emulsion formulation.
- Dexmedetomidine provides targeted sedation in the ICU without causing significant respiratory depression, making it highly effective for patients weaning off the ventilator.
Sedation management directly links to ICU delirium. Intensive care unit (ICU) delirium is associated with prolonged mechanical ventilation and increased patient mortality. We assess for this daily because the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) is a standardized screening tool used to detect delirium.
To combat delirium and muscle wasting, early mobility protocols in the intensive care unit reduce the incidence and duration of patient delirium. Alongside mobility, metabolic support is vital: enteral nutrition should be initiated within 24 to 48 hours of intensive care unit admission for hemodynamically stable patients to preserve gut mucosa.
Communication
When care complexity scales up, communication must be standardized. The SBAR communication model standardizes critical information transfer among healthcare providers.
- SBAR stands for Situation, Background, Assessment, and Recommendation.
Practicing critical care in Saudi Arabia means aligning life-saving interventions with national bioethics and Islamic jurisprudence (Fatwa).
When medical intervention becomes futile, Do Not Resuscitate (DNR) orders in Saudi Arabia require the written agreement of three consultant physicians according to Islamic fatwa guidelines. It is critical to understand that a Do Not Resuscitate (DNR) order prohibits CPR but requires the continuation of standard medical nursing care and comfort measures. We do not stop caring for the patient; we simply shift the focus from resuscitation to palliation.
Finally, when neurological damage is catastrophic and irreversible, a formal determination of death may be required. The formal declaration of brain death in Saudi Arabia requires two separate clinical examinations conducted by specialized physicians, ensuring absolute diagnostic certainty before the withdrawal of life support or organ procurement can be considered.