Surgical Nursing
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Surgery is a meticulously orchestrated physiological crisis. When a patient is wheeled into the operating theater, the surgical team intentionally overrides the body’s innate defense mechanisms—breaching the skin, suspending consciousness, and manipulating internal hemodynamics—to excise, repair, or reconstruct. For the nurse preparing for the Saudi Nursing Licensure Examination (SNLE), perioperative care cannot be viewed as a mere checklist of disconnected tasks. It is the continuous, rigorous management of a patient's transition across three distinct biological states: the preoperative preparation, the intraoperative trauma, and the postoperative recovery.
To master this subject, you must understand the why behind every clinical intervention. We do not just measure vital signs; we track the body's compensatory mechanisms as they fight to restore homeostasis.
Before a patient ever encounters a scalpel, the foundations of surgical safety are laid. Think of the preoperative phase as calibrating a highly complex machine before pushing it past its operational limits.
The Anatomy of Informed Consent
We must begin with legal and ethical safety. Many assume consent is merely the physical act of signing a document. It is not. Informed consent represents the patient's voluntary agreement to undergo a surgical procedure based on full disclosure of risks.
Because the surgeon intimately understands the procedure’s specific anatomical risks, the physician performing the surgical procedure is legally responsible for obtaining informed consent.
So, what is the nurse doing in the room? The nurse's role during informed consent is strictly to witness the patient's signature. However, "witnessing" demands acute clinical judgment. As the witness, the nurse must verify that the patient is mentally competent prior to signing the surgical consent form and must verify that the patient is signing the surgical consent form voluntarily, free from familial or medical coercion.
Metabolic and Pharmacological Preparation
Anesthesia suppresses protective airway reflexes. If the stomach is full, gastric contents can be regurgitated and aspirated into the lungs, causing catastrophic pneumonitis. Therefore, gastric emptying is highly regulated. The American Society of Anesthesiologists guidelines dictate fasting from clear liquids for at least two hours before elective surgery. Solids take longer to transit: patients must fast from a light meal for at least six hours, and fast from a heavy or fatty meal for at least eight hours before elective surgery.

Medication management requires a delicate balancing act between hemorrhage and systemic shock:
- Anticoagulant medications are typically discontinued five to seven days before elective surgery to prevent excessive bleeding. We must let the body's natural clotting cascade rebuild.
- Conversely, beta-blocker medications are generally continued on the morning of surgery to prevent perioperative cardiac events. The physiological stress of an incision causes a massive sympathetic nervous system surge; beta-blockers act as the chemical brakes on the myocardium, preventing sudden tachycardia or ischemia.
The Final Preoperative Checklist
In the hours immediately before the transfer, the nurse finalizes patient safety variables. The preoperative checklist requires the removal of all patient jewelry before transfer to the operating room. Why? Because metal jewelry conducts electricity and can cause severe thermal burns when intraoperative electrocautery is used.
To arm the patient against postoperative complications, education happens now, while the patient is lucid. Teaching deep breathing exercises preoperatively ensures the patient knows how to reduce the risk of postoperative atelectasis once they wake up in pain.
Finally, to combat site infection, prophylactic surgical antibiotics are optimally administered within 60 minutes before the surgical incision, ensuring peak tissue concentration exactly when the scalpel breaks the skin barrier.
Once inside the operating room, the environment is rigidly divided by the sterile field.

Navigating the Sterile Field
Every professional in the room has geographically defined boundaries:
- The scrub nurse functions entirely within the sterile field during a surgical procedure, passing instruments directly into the surgical site.
- The circulating nurse functions entirely outside the sterile field. They are the macro-managers of the room's environment and safety. Because they can move freely, the circulating nurse is responsible for documenting all intraoperative nursing activities.
The circulating nurse also manages the electrocautery equipment. To safely disperse the electrical current entering the patient's body from the surgical cautery pen, the circulating nurse verifies that the electrocautery grounding pad is securely attached to the patient. To ensure uniform electrical dispersion and prevent thermal burns, the electrocautery grounding pad must be placed on a well-muscled body area free of hair. Fat and hair are poor conductors; well-perfused muscle provides a safe exit path for the electrical current.
Furthermore, because the anesthetized patient cannot feel pressure or pain, correct patient positioning during surgery prevents intraoperative peripheral nerve injury.
The WHO Surgical Safety Checklist
The operating room is a high-stakes environment where assumptions lead to fatalities. The World Health Organization Surgical Safety Checklist consists of three phases known as sign-in, time-out, and sign-out.
The most critical of these for the SNLE is the "time-out." The surgical time-out phase occurs immediately before the skin incision. To ensure zero ambiguity, the entire surgical team must actively participate in the surgical time-out.
During this synchronized pause, the team collectively halts to verify three absolute truths:
- The surgical time-out process confirms the correct patient identity.
- The surgical time-out process confirms the correct surgical site.
- The surgical time-out process confirms the correct surgical procedure.
The Threat of Malignant Hyperthermia
During anesthesia, the nurse must remain highly vigilant for a rare but lethal crisis. Malignant hyperthermia is a severe hypermetabolic reaction to specific anesthetic agents.
Certain drugs cause the skeletal muscle calcium channels to lock open in genetically susceptible individuals, sending muscle metabolism into a catastrophic overdrive.
- The paralytic medication succinylcholine is a known pharmacological trigger for malignant hyperthermia.
- Similarly, inhaled halogenated anesthetics can trigger malignant hyperthermia in susceptible patients.
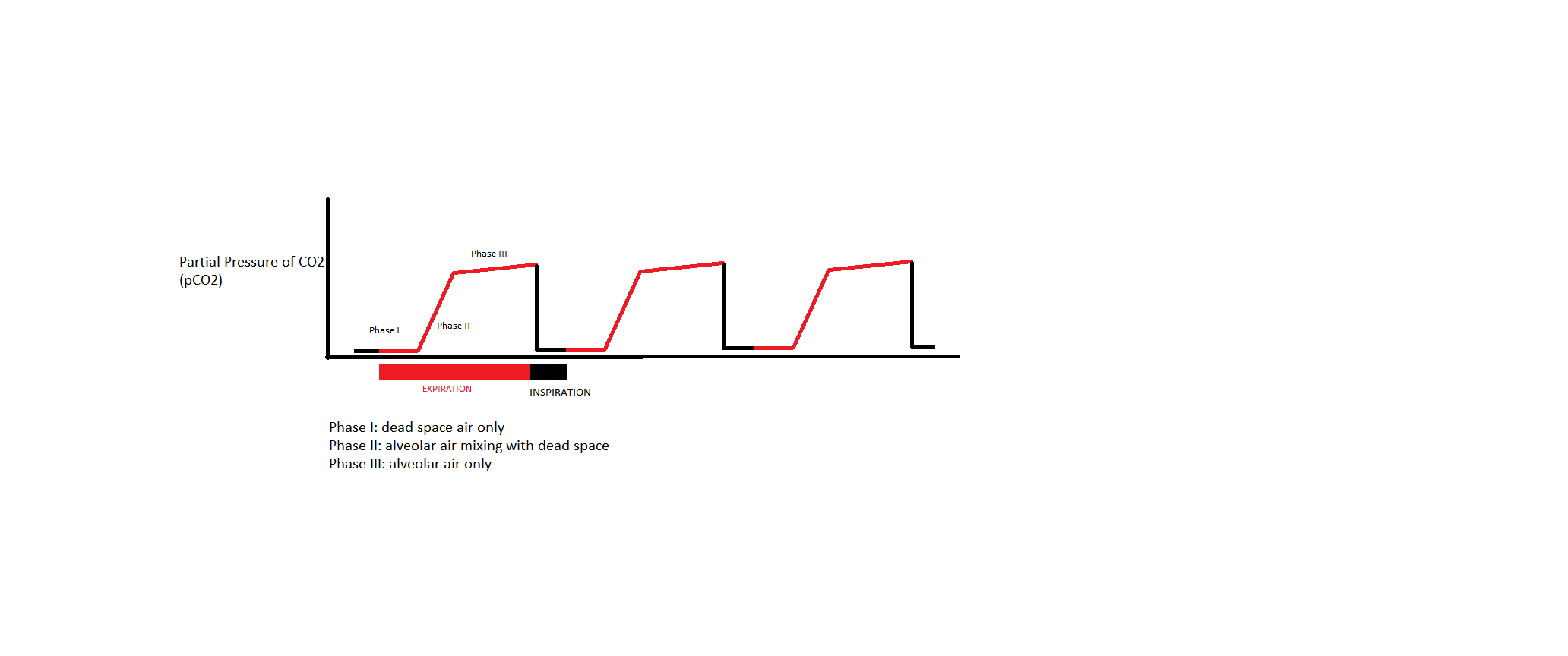
Because the muscles are rapidly burning oxygen and creating waste, an early clinical sign of malignant hyperthermia is an unexplained increase in end-tidal carbon dioxide. This occurs long before you see a spike in core body temperature. Another defining, classic early sign is muscle rigidity of the masseter muscle (jaw clenching).
Clinical Rescue: If you see these signs, anesthesia is immediately halted. Dantrolene sodium is the specific pharmacological antidote for malignant hyperthermia, acting directly to stop the release of calcium within the muscle cells.
The physiological assault has ended, but the recovery of homeostasis has just begun.
The Post-Anesthesia Care Unit (PACU)
When the patient rolls into the PACU, their central nervous system is heavily depressed. Therefore, the absolute primary goal in the Post-Anesthesia Care Unit is maintaining a patent patient airway. Every other assessment is secondary to oxygenation.
How do we know when the patient's central nervous system has safely rebooted? The Aldrete scoring system evaluates a patient's physiological readiness for discharge from the Post-Anesthesia Care Unit. It assesses respiration, oxygen saturation, consciousness, circulation, and activity. An Aldrete score of eight or higher typically indicates readiness for discharge from the Post-Anesthesia Care Unit.
Hemodynamic Monitoring: Catching Hemorrhage
On the surgical ward, the nurse acts as a hemodynamic detective. If an internal suture slips, blood will pool silently inside the body cavity.
How does the body react to losing blood? Before the blood pressure ever drops, the heart beats faster to compensate for the lost stroke volume. Therefore, postoperative tachycardia is often the first clinical indicator of internal surgical hemorrhage.
If you wait for the blood pressure to plummet, you have waited too long. Postoperative hypotension is considered a late clinical sign of hypovolemic shock, indicating that the body's compensatory mechanisms have entirely failed.
Respiratory Recovery
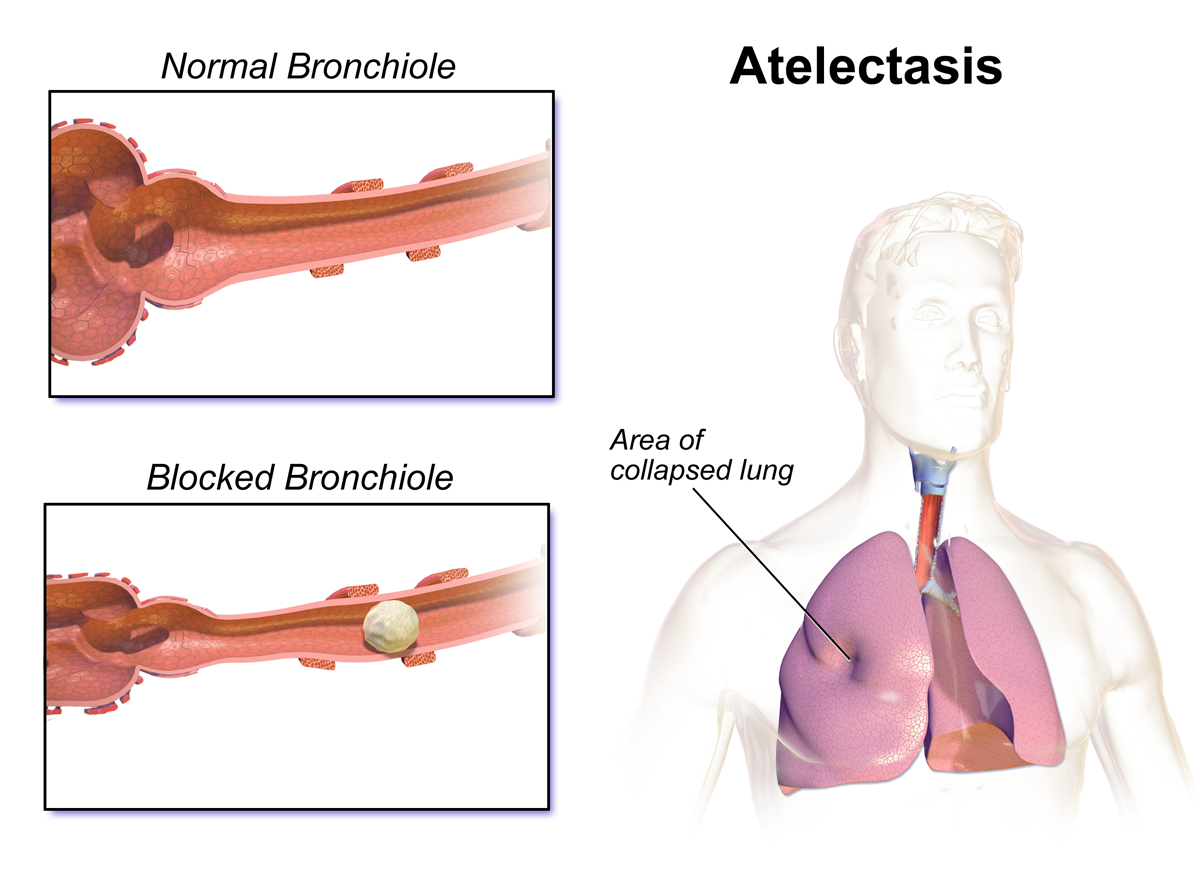
Anesthesia and pain cause patients to take shallow breaths. This leads to collapsed alveolar sacs in the bases of the lungs.
- A low-grade fever during the first 48 hours postoperatively is most typically caused by pulmonary atelectasis.
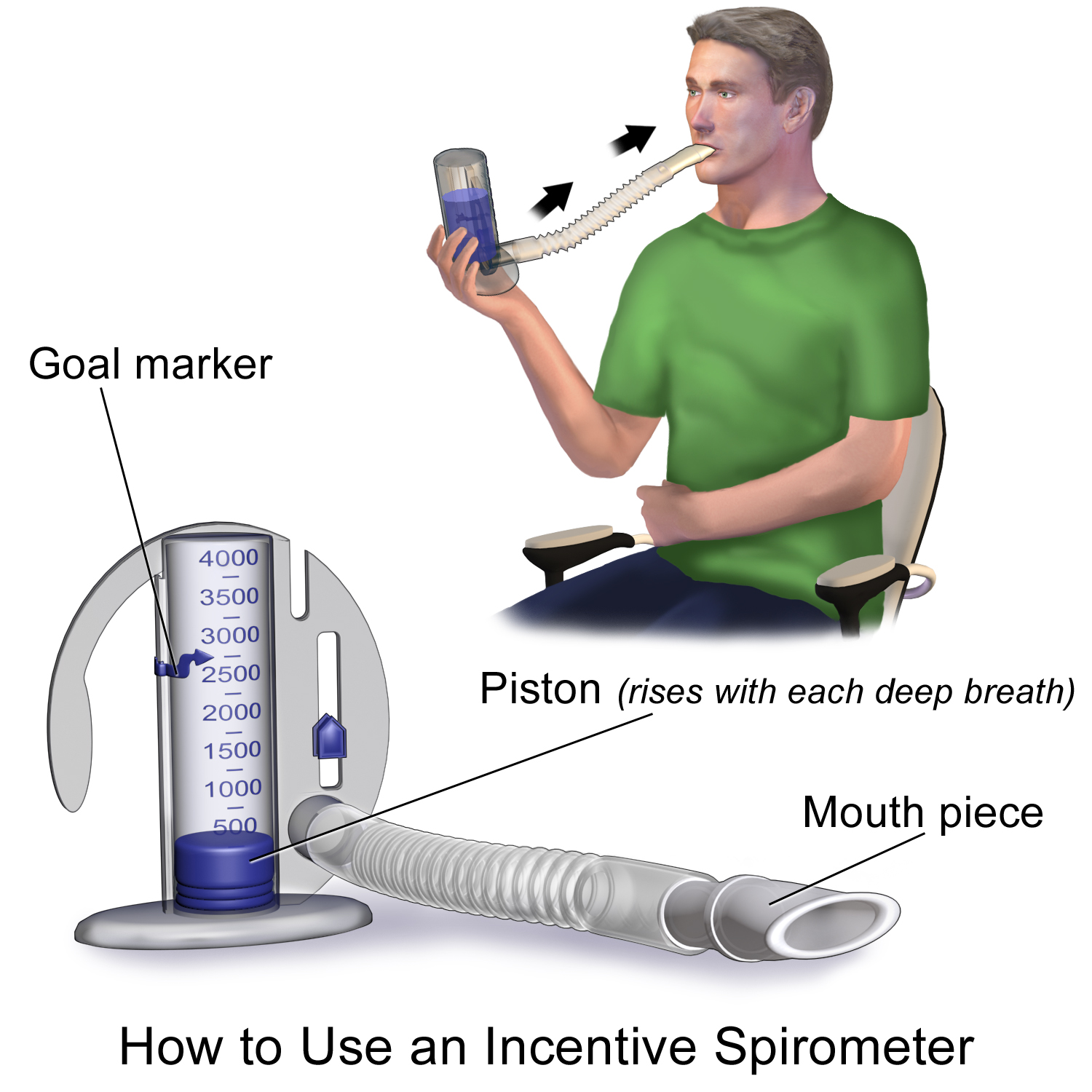
- To reverse this, we use mechanical expansion: Incentive spirometry encourages maximum alveolar inflation to prevent postoperative pulmonary complications.
- To be effective, postoperative patients should optimally perform incentive spirometry ten times every hour while awake.
Because deep breathing stretches the fresh abdominal incision, it hurts. Splinting the surgical incision with a pillow minimizes abdominal pain during coughing exercises, providing counter-pressure that gives the patient the confidence to fully expand their lungs.
Gastrointestinal and Genitourinary Resuscitation
Anesthesia essentially puts the gut and bladder to sleep. Postoperative paralytic ileus is the temporary cessation of intestinal peristalsis following surgery. If the nurse auscultates the abdomen and notes absent bowel sounds on postoperative day two, this indicates a potential paralytic ileus.
How do we definitively know the gut has woken up? Listening to bowel sounds can be deceptive (you might just be hearing fluid shifting). Instead, passing flatus is the most reliable clinical indicator of returning gastrointestinal motility after abdominal surgery.
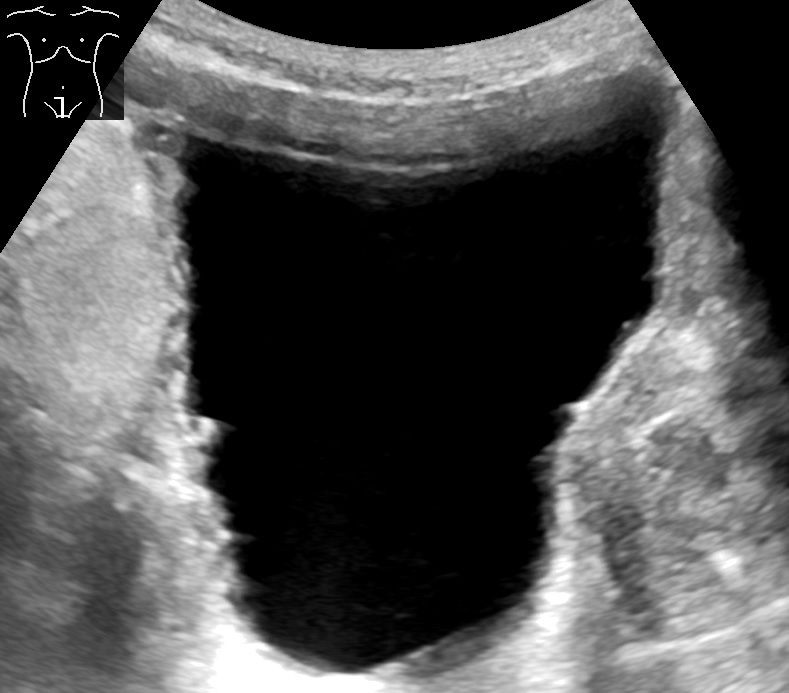
Similarly, the bladder detrusor muscle can remain sluggish. Postoperative urinary retention is defined as the inability to void within six to eight hours after surgery. If the patient feels fullness but cannot void, do not immediately rush to insert a catheter. A bladder ultrasound scan is the first non-invasive intervention to assess suspected postoperative urinary retention, allowing you to quantify the urine volume objectively.
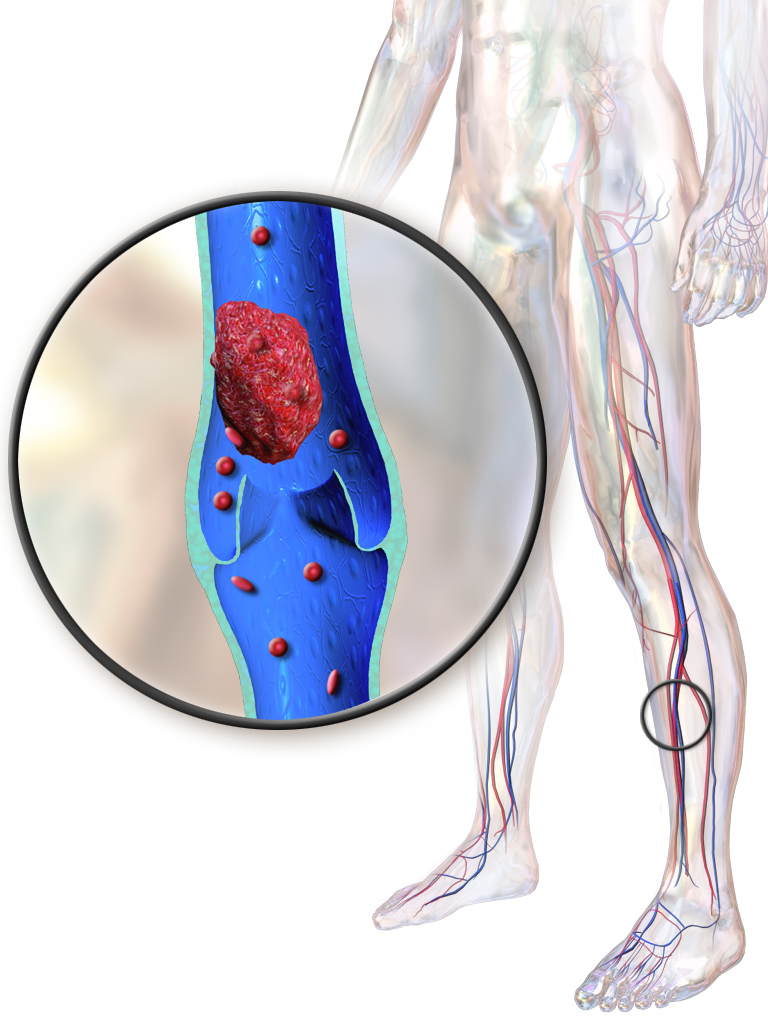
Deep Vein Thrombosis (DVT) Prophylaxis
Surgery triggers the inflammatory cascade, making the patient's blood hypercoagulable. Combine this with bedrest (venous stasis), and you have a perfect recipe for a DVT.
- Sequential compression devices are applied to the postoperative patient's lower extremities to prevent venous stasis by mechanically mimicking the pumping action of calf muscles.
- Chemically, low-molecular-weight heparin is commonly prescribed postoperatively to prevent venous thromboembolism.
- However, the most effective intervention is simply gravity and movement: early postoperative ambulation significantly reduces the risk of developing a deep vein thrombosis.
Wound Management and Surgical Drains
Surgical incisions have predictable timelines for complications. While atelectasis causes early fevers, postoperative surgical wound infections typically manifest on postoperative days three to five.
To prevent hematomas or seromas from forming under the skin and inviting infection, surgeons often place closed-suction drains. A Jackson-Pratt drain operates using continuous negative suction pressure to remove surgical wound fluid. To ensure the physics of this device actually work, the nurse must completely compress the Jackson-Pratt drain bulb before replacing the plug to establish proper suction. If the bulb is fully expanded, it is doing absolutely nothing.

Wound Failure: Dehiscence and Evisceration
Sometimes, the structural integrity of the incision fails. Wound dehiscence is the partial or complete separation of the outer surgical wound layers. Patients will often intuitively recognize this mechanical failure; a sudden popping sensation in the abdomen postoperatively often precedes surgical wound dehiscence.

A far more severe catastrophe is wound evisceration: the protrusion of internal abdominal organs through an opened surgical incision. This is a dire surgical emergency.
- First, do no harm: The nurse must never attempt to push eviscerated internal organs back into the abdominal cavity. Doing so risks catastrophic bowel perforation and profound sepsis.
- Second, protect the exposed tissue: Immediate nursing management for wound evisceration requires covering the protruding organs with sterile saline-soaked dressings to prevent the tissue from drying out and necrotizing.
- Third, reduce mechanical tension: The nurse must place a patient with an eviscerated wound in a low Fowler's position with flexed knees. Elevating the knees immediately relaxes the abdominal rectus muscles and fascia, preventing further visceral extrusion while awaiting emergency surgical intervention.