Pediatric Medical
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
To understand pediatric nursing is to understand the physics of a system in constant, rapid acceleration. A child is not simply a miniature adult, just as a caterpillar is not a miniature butterfly; they are entirely different biological entities operating under unique developmental rules. When a nurse walks into a pediatric ward in Riyadh or Jeddah, they are stepping into a laboratory of human maturation. The respiratory structures are disproportionately narrow, the fluid volumes are precariously balanced, and the neurological systems are actively wiring themselves in real time. Mastering this dynamic environment for the SNLE requires more than memorizing a checklist of milestones and diseases. It requires seeing how physiological vulnerabilities intersect with a child’s expanding cognitive world.
If you want to evaluate a child's health, you must first measure their velocity. Growth in the first year of life is an explosive event. A healthy infant is essentially a machine designed to convert milk into mass.
To track this, we look at the weight and the skull. An infant's birth weight typically doubles by six months of age and triples by twelve months of age. The cranium, needing to accommodate a rapidly expanding brain, is built with expansion joints called fontanels. The posterior fontanel normally closes between two and three months of age, while the larger anterior fontanel normally closes between twelve and eighteen months of age.

Motor and Cognitive Mechanics
Physical milestones follow a strict cephalocaudal (head-to-toe) and proximodistal (center-outward) blueprint.
- By five months, the infant achieves enough core strength to roll from front to back.
- By eight months, spinal control allows the infant to sit unsupported.
- By nine months, fine motor coordination emerges, and the infant develops a crude pincer grasp, allowing them to pick up small objects (which they will inevitably put in their mouths).
By the end of the first year, the child transitions to a toddler, shifting from stationary observation to active exploration. A toddler typically walks without assistance by fifteen months of age. Language and coordination scale together: a child typically speaks in two-to-three word sentences by two years of age and can usually walk up and down stairs. By the time they reach three years of age, a child can usually ride a tricycle, demonstrating complex bilateral coordination. Once they hit the school-age years, the explosive growth steadies out; school-age children typically grow an average of two inches per year.
The Psychosocial Framework: Erikson and Piaget
Understanding a child's mind is critical for effective nursing care. Jean Piaget's cognitive theory defines the first two years of life as the sensorimotor stage—the child learns about the universe strictly through touching, tasting, and moving.
Erik Erikson provided the psychosocial map of human development, and you must know this for the SNLE:
| Age Group | Erikson's Stage | Clinical Implication in the Ward |
|---|---|---|
| Infancy | Trust versus Mistrust | Needs must be met consistently. Comfort and feeding build a secure foundation. |
| Toddler | Autonomy versus Shame and Doubt | They want control. Offer safe, simple choices (e.g., "Do you want the red cup or the blue cup for your medicine?"). |
| Preschool | Initiative versus Guilt | They are curious and magical thinkers. They need to explore without feeling reprimanded for their natural curiosity. |
| School-Age | Industry versus Inferiority | They want to learn and accomplish tasks. Praise their cooperation and explain how things work. |
| Adolescence | Identity versus Role Confusion | Peer acceptance and self-image are paramount. |
Because cognitive development is tied to age, separation anxiety typically begins to manifest around six months of age as the infant realizes they are a separate entity from their caregiver and that the caregiver can disappear.
Play and Procedural Communication
Play is the serious work of childhood. It is how they test the physics of their world and social dynamics.
- Toddlers engage in parallel play: they sit side-by-side playing with their own toys without interacting.
- Preschoolers advance to associative play: playing together without strict rules or a unified goal.
- School-age children develop cooperative play: involving organized rules and team goals.

When we explain medical procedures, we must match our communication to their cognitive stage.
- Explaining medical procedures to a toddler should occur immediately before the procedure to minimize anticipatory anxiety.
- Explaining medical procedures to preschool children should involve simple terms and medical play (letting them handle a stethoscope or mask).
- Explaining medical procedures to school-age children should include scientific rationales—they want to know why the blood is being drawn and how the machine works.
- Adolescents should be provided privacy and opportunities to speak with healthcare providers without parents present, honoring their need for identity and autonomy.
Pediatric prevention relies on specific nutritional and safety protocols. The ideal fuel for the first half-year is highly specific. Exclusive breastfeeding is recommended for the first six months of an infant's life. When it is time to upgrade their diet, solid foods are typically introduced around six months of age, and iron-fortified rice cereal is typically the first solid food introduced because it is easily digestible and replenishes depleting iron stores.
Crucial Warning: Cow's milk is contraindicated in infants under one year due to the risk of intestinal bleeding and iron deficiency. Their GI tract simply cannot process the heavy protein load of bovine milk.
Environmental and Immunological Armor
To protect the infant while sleeping, infants should be placed flat on their backs for sleep to reduce the risk of Sudden Infant Death Syndrome (SIDS). In transport, children must ride in a rear-facing car seat until they are at least two years old or reach the seat's maximum limit, because their heavy heads and weak cervical ligaments are incredibly vulnerable to whiplash forces.

Immunizations are the software updates for the pediatric immune system. You must know two critical ones for the SNLE:
- The rotavirus vaccine is administered orally to infants to prevent severe gastroenteritis, a leading cause of pediatric dehydration.
- The measles, mumps, and rubella (MMR) vaccine is typically first administered between 12 and 15 months of age because maternal antibodies interfere with live vaccines if given too early.
Because children have a higher surface-area-to-volume ratio, they lose water rapidly. In the Saudi climate, fluid status is a daily nursing priority. Dehydration in infants is commonly assessed through the frequency of wet diapers. If the fluid level drops significantly, you will see a structural change in the skull: a sunken anterior fontanel is a clinical sign of moderate to severe dehydration in infants.
If the child is dehydrated, do not immediately rush for the IV. Oral rehydration therapy is the first-line treatment for mild to moderate pediatric dehydration, utilizing precise sodium-glucose cotransport mechanisms in the gut to pull water into the bloodstream.
Structural GI Emergencies
Sometimes the GI "plumbing" is structurally flawed:
- Pyloric Stenosis: The sphincter exiting the stomach becomes hypertrophied (thickened). Because food cannot pass into the intestines, pressure builds. This classically presents with projectile vomiting immediately after feeding, and upon palpation, you will feel an olive-shaped mass in the right upper quadrant.
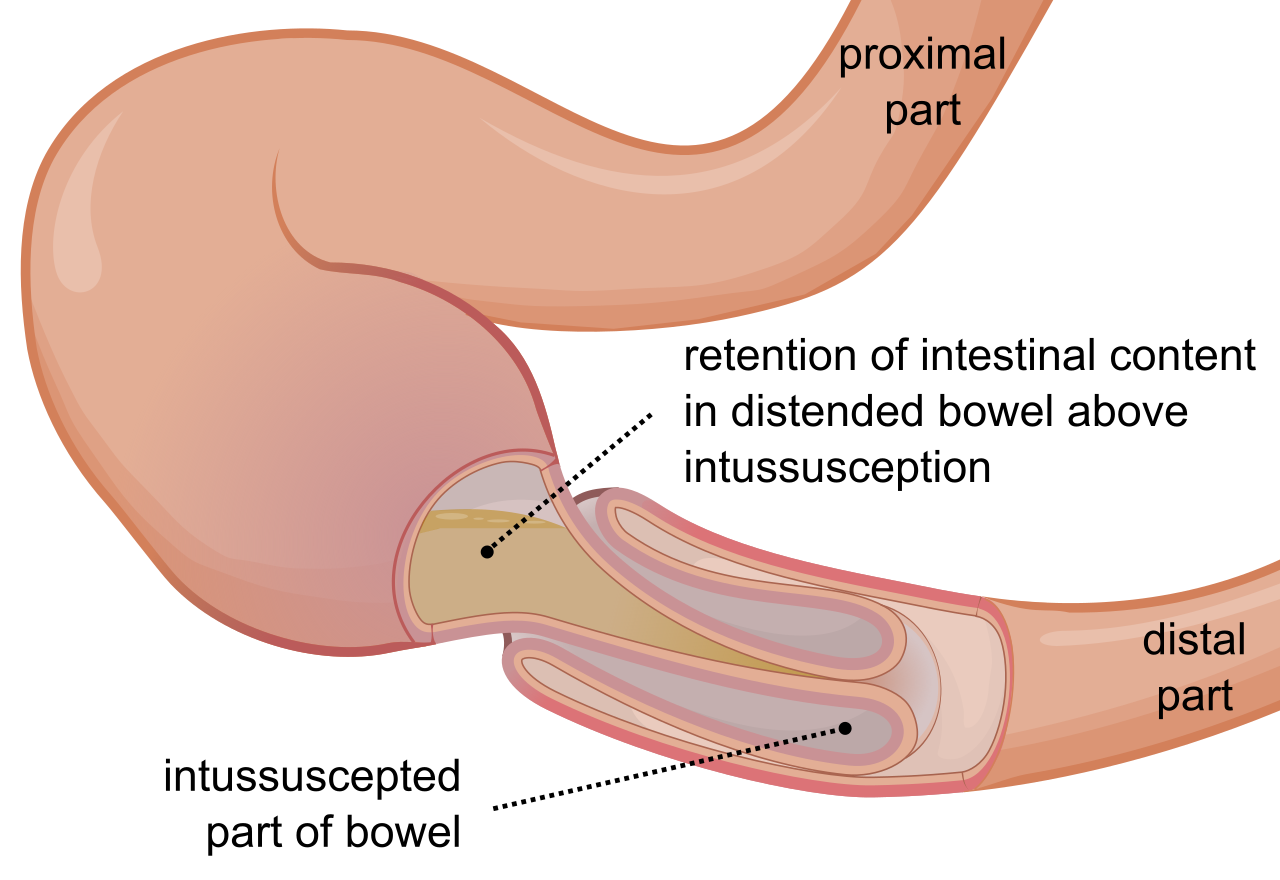
- Intussusception: This is a mechanical crisis where one bowel segment telescopes into an adjacent segment, cutting off blood supply. The friction and ischemia produce mucin and blood, resulting in the classic clinical manifestation: currant jelly stools.
- Hirschsprung Disease: This is a neurological defect of the gut. It is characterized by the absence of ganglion cells in the colon, meaning peristalsis stops at that segment. A key diagnostic red flag is the failure to pass meconium within the first 48 hours of life.
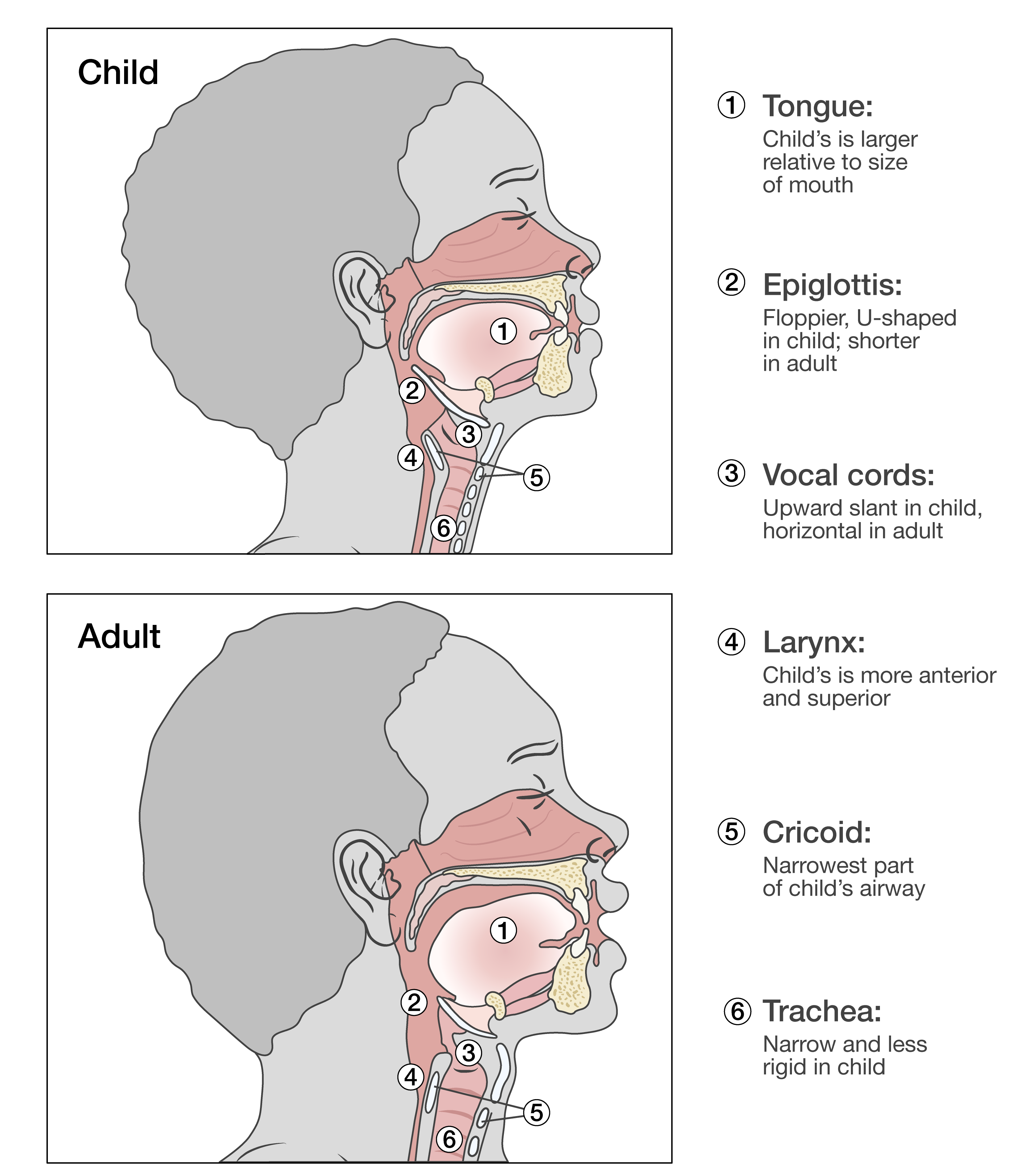
A child's airway is roughly the diameter of their pinky finger. Even a millimeter of edema exponentially increases airway resistance.
Upper Airway Crises
- Croup: A viral infection of the larynx and trachea. It is instantly recognizable and characterized by a distinctive barking cough and inspiratory stridor (a high-pitched whistling sound as air pulls through a swollen trachea).
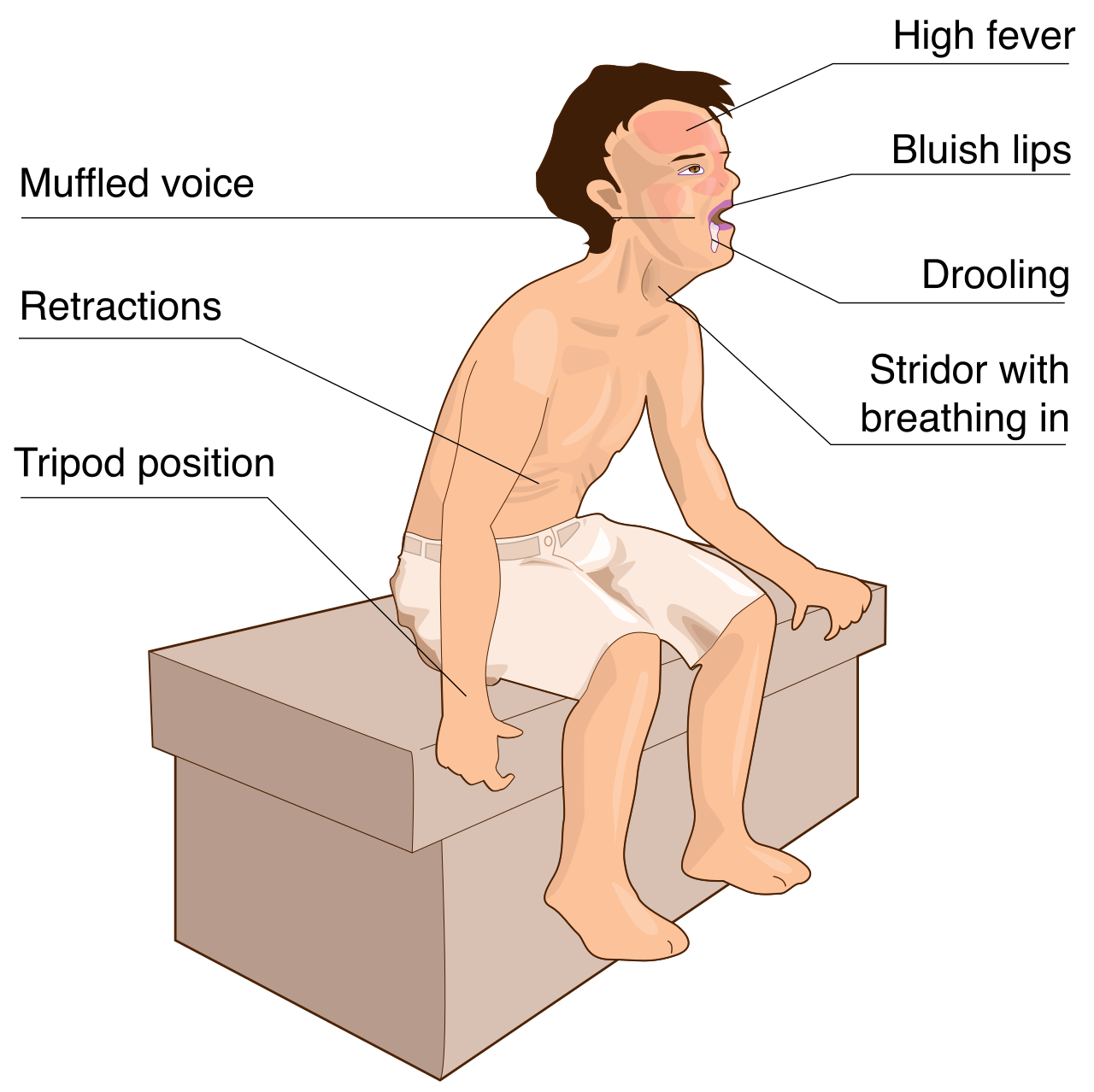
- Epiglottitis: This is an absolute pediatric medical emergency requiring immediate airway management. A bacterial infection causes the epiglottis to swell like a cherry, threatening to completely occlude the trachea. A child with epiglottitis typically assumes the tripod position (leaning forward, chin thrust out) to mechanically facilitate breathing.
Never forget: Throat inspection with a tongue depressor is strictly contraindicated in a child with suspected epiglottitis. The mechanical stimulation can trigger an instant, fatal laryngospasm.
Lower Airway and Chronic Conditions
- Bronchiolitis: Inflammation of the tiny bronchioles. Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis in children under two years old, generating massive amounts of thick secretions that infants cannot clear.
- Asthma: A hyper-reactive airway disease. It is a chronic inflammatory disorder of the airways causing wheezing and breathlessness, often requiring bronchodilators and inhaled corticosteroids.
- Cystic Fibrosis (CF): A systemic genetic defect. Cystic fibrosis is an autosomal recessive disorder causing thick mucus production in the respiratory and gastrointestinal tracts. Because the mucus is so thick, it blocks the pancreatic ducts. To digest food, pancreatic enzymes must be administered with every meal and snack to children with cystic fibrosis. To diagnose CF, we look at the sweat glands: A sweat chloride test is the primary diagnostic tool.
When the embryonic heart fails to fold correctly, we see congenital anomalies.
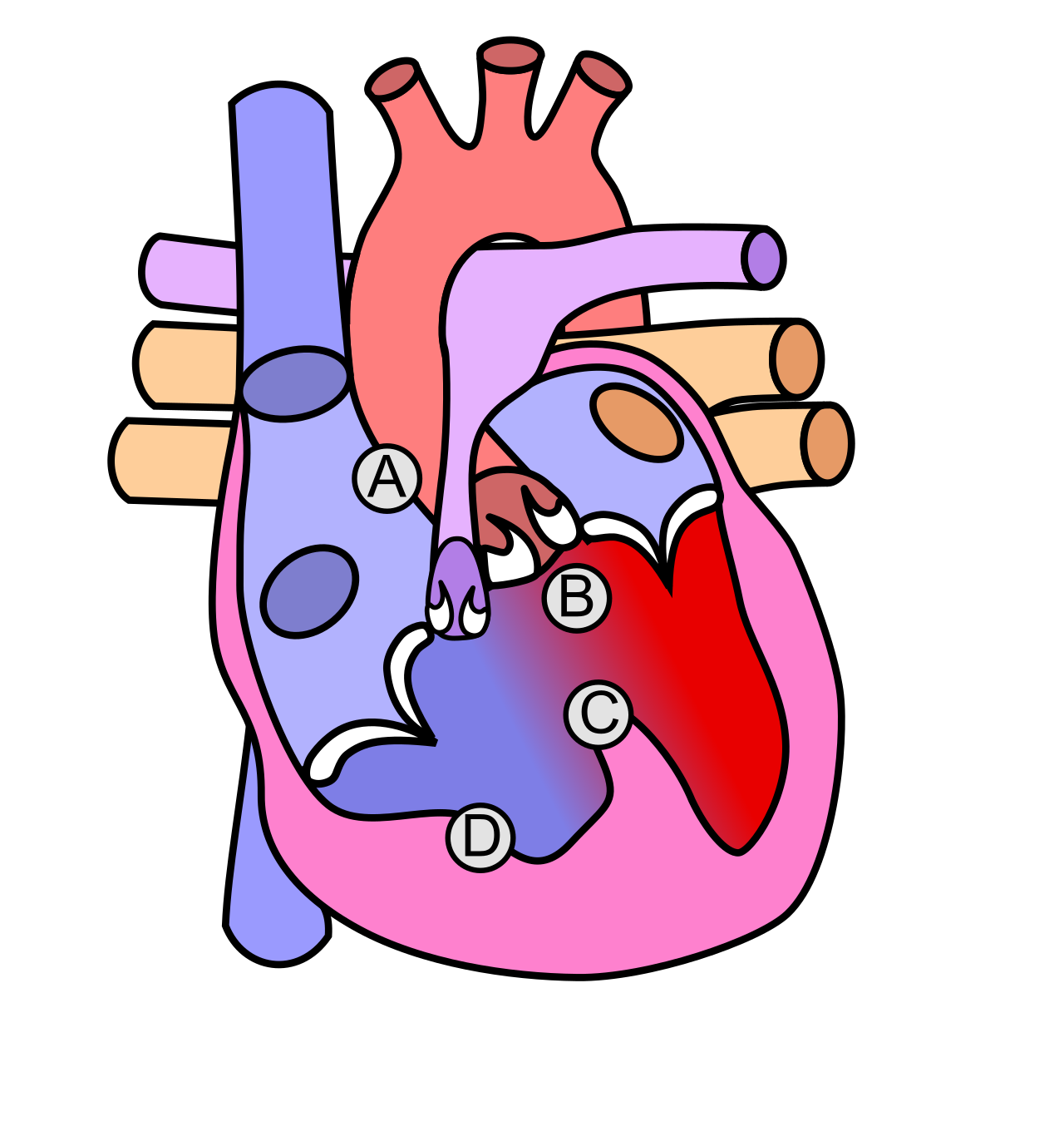
Tetralogy of Fallot is the classic cyanotic heart defect. It includes four distinct flaws: a ventricular septal defect, pulmonary stenosis, overriding aorta, and right ventricular hypertrophy. Because blood flow to the lungs is restricted by the pulmonary stenosis, infants can experience "Tet spells," which are hypercyanotic episodes occurring during crying or feeding. The immediate nursing intervention is mechanical: Placing an infant in a knee-to-chest position increases systemic vascular resistance to relieve a Tet spell, forcing more blood back through the pulmonary artery to be oxygenated.
Acquired Cardiovascular Diseases
- Rheumatic Fever: This autoimmune, inflammatory disease damages heart valves. It typically develops two to six weeks after an untreated group A streptococcal pharyngitis (strep throat).
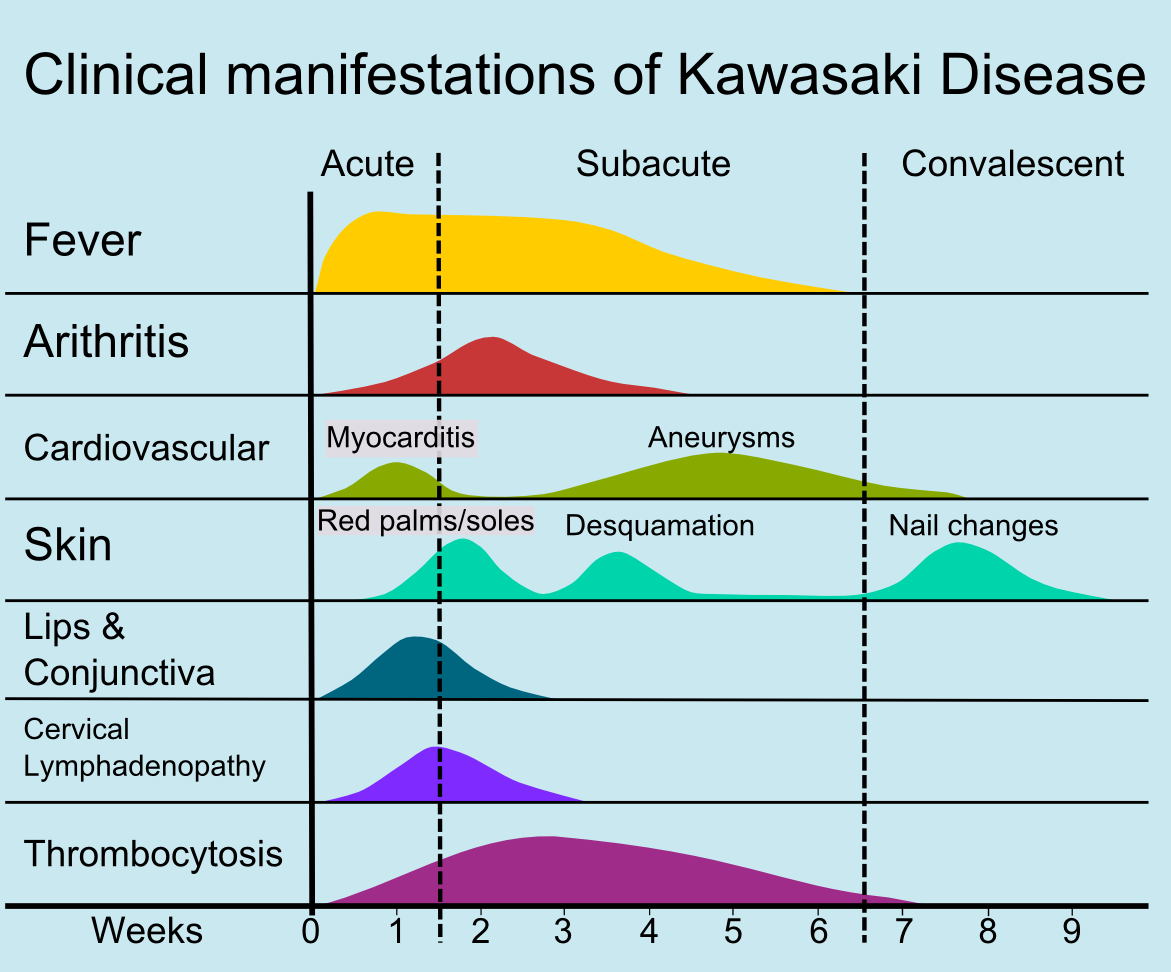
- Kawasaki Disease: An acute systemic vasculitis primarily affecting children under five years old. You will see a high fever, peeling skin, and a classic strawberry tongue. The primary danger is that the inflammation targets the coronary arteries.
Treating Kawasaki requires an exception to a major pediatric rule. Normally, aspirin is generally contraindicated in pediatric populations due to the risk of Reye syndrome (a fatal encephalopathy and liver failure). However, in Kawasaki disease, aspirin is indicated for its anti-inflammatory and antiplatelet effects. Alongside this, intravenous immunoglobulin (IVIG) is a standard treatment for Kawasaki disease to prevent coronary artery aneurysms.
The pediatric brain is hyper-excitable. Because the hypothalamus is immature, rapid temperature changes can cause electrical storms in the brain. Febrile seizures typically occur in children between six months and five years of age, and it is critical to explain to panicked parents that febrile seizures are triggered by a rapid rise in body temperature rather than the absolute peak temperature.
Infection and Pressure in the CNS
- Meningitis: Bacterial infection of the meninges. To test for meningeal irritation in children, we look for two mechanical reflexes: Kernig's sign (pain on knee extension) and Brudzinski's sign (neck flexion causes involuntary hip/knee flexion). If suspected, a lumbar puncture is the definitive diagnostic procedure for pediatric bacterial meningitis.
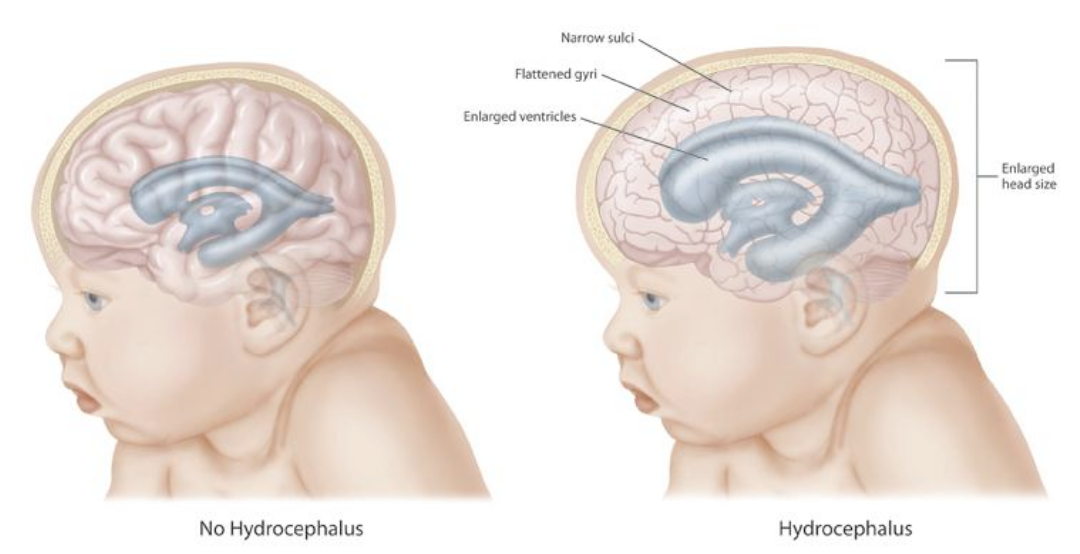
- Hydrocephalus: A plumbing issue of the brain, characterized by an abnormal accumulation of cerebrospinal fluid in the brain ventricles. Because an infant's cranial sutures have not fused, a rapidly increasing head circumference is a primary sign of hydrocephalus in infants.
Renal Disorders: Losing the Filter
- Acute post-streptococcal glomerulonephritis (APSGN): Occurs after a strep infection clogs the glomerular filter with antigen-antibody complexes. It classically presents with gross hematuria (tea-colored urine) and periorbital edema.
- Nephrotic Syndrome: The glomerular membrane becomes excessively permeable to proteins. It is characterized by massive proteinuria, hypoalbuminemia, and severe edema. Because the albumin is lost in the urine, vascular fluid leaks into the interstitial spaces, causing the extreme swelling.
The bone marrow and blood are susceptible to genetic and malignant disruptions.
- Acute Lymphoblastic Leukemia (ALL): The rampant overproduction of immature white blood cells. It is the most common childhood cancer.
- Hemophilia A: An X-linked recessive bleeding disorder caused by a deficiency in coagulation factor VIII. Because it is X-linked, it almost exclusively affects males, requiring lifelong factor replacement.
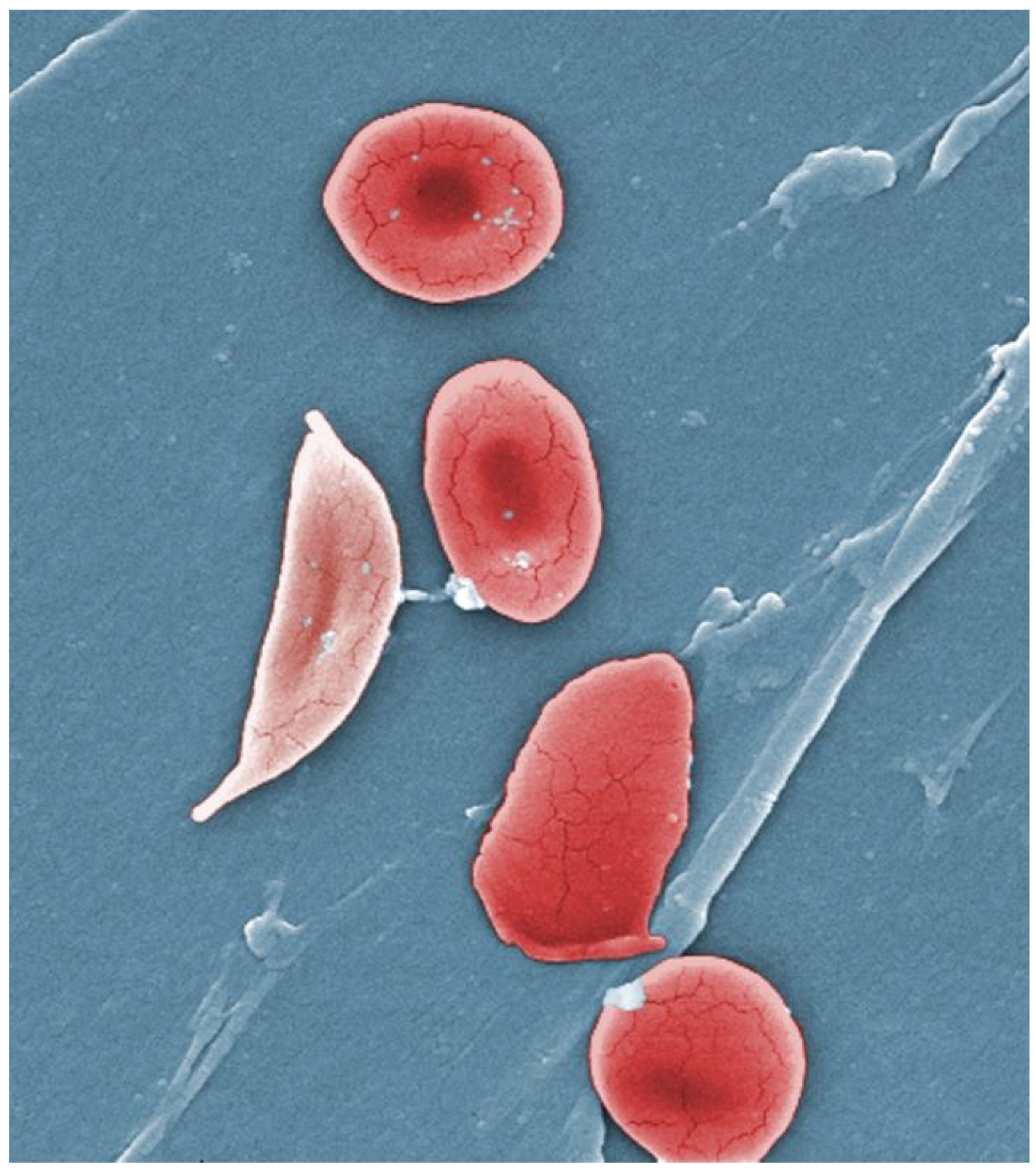
- Sickle Cell Anemia: An autosomal recessive genetic disorder affecting hemoglobin structure. Under stress, the red blood cells collapse into a rigid sickle shape, blocking capillaries. Vaso-occlusive crises in sickle cell anemia are primarily triggered by hypoxia, dehydration, or infection. When a child presents in crisis to the ER, the tissue ischemia causes excruciating pain. Therefore, pain management and aggressive hydration are the primary nursing interventions for a vaso-occlusive crisis, diluting the blood and flushing out the microvascular blockages.
In your daily practice across Saudi Arabia, and as you sit for your SNLE, view every pediatric case through this lens. You are not just treating a disease; you are protecting a rapidly evolving biological system. Whether it is shielding a toddler's airway from a tongue depressor during epiglottitis, or teaching a parent why their child with Kawasaki needs aspirin despite what they read online, your interventions safeguard the delicate physics of human growth.