Pediatric Surgical
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
A pediatric surgical patient is not simply a miniature adult, but a fundamentally distinct physiological system operating under entirely different thermodynamic, metabolic, and psychological rules. When a child is transferred to the operating theater, the margins for error compress significantly. Airway diameters are measured in millimeters, fluid shifts in milliliters, and therapeutic windows are exquisitely narrow. To manage perioperative care for a pediatric patient is to master the intersection of developmental psychology, precision pharmacology, and applied physics. Success on the Saudi Nursing Licensure Examination (SNLE) and in clinical practice across the Kingdom requires a deep, intuitive grasp of how to protect these vulnerable patients from the moment of surgical consent to their final discharge from the recovery unit.
Before a scalpel is ever lifted, the groundwork for a safe surgical intervention must be laid through rigorous legal protocols and developmentally targeted psychological preparation.
Surgical Consent in Saudi Arabia
Consent is the legal and ethical authorization for invasion of the body. In Saudi Arabia, the legal age for an individual to provide independent surgical consent is 18 years. Consequently, for the vast majority of pediatric surgical cases, a parent or legal guardian must sign the surgical consent form for any patient under 18 years of age in Saudi Arabia. Without this documented authorization, the procedure cannot proceed outside of immediate, life-and-death emergencies.
Deconstructing Preoperative Anxiety
A hospital is an alien landscape to a child, and anxiety manifests differently depending on the maturity of the patient's nervous system. Preoperative separation anxiety reaches its peak intensity during the toddler years. For these toddlers, the fundamental terror is the loss of their primary caregiver. We mitigate this by allowing parents to accompany their child into the anesthetic induction room, an intervention proven to substantially reduce the child's preoperative anxiety levels before they drift to sleep.
As cognitive capacity expands, so must our educational approach. Developmentally appropriate preoperative teaching for a preschool-aged child focuses primarily on expected sensory experiences. A four-year-old does not possess the abstract reasoning to understand a hernia repair, but they need to know that the anesthetic mask will smell like bubblegum, the monitors will beep like a video game, and their throat might feel scratchy afterward.
For older children, we bridge the cognitive gap using therapeutic play, which utilizes actual medical equipment like syringes and stethoscopes to familiarize a child with upcoming surgical procedures. By touching and manipulating the tools that will be used on them, the child regains a locus of control, transforming a terrifying medical implement into a comprehensible object.
The Pharmacological Bridge
When psychological interventions are insufficient, pharmacology provides a bridge to safety. Oral midazolam is the most common anxiolytic medication administered to pediatric patients prior to surgery. It provides reliable sedation and anterograde amnesia, easing the transition into the operating room.
Simultaneously, we must protect the child from the trauma of needle punctures. Eutectic mixture of local anesthetics (EMLA) cream requires a minimum of 60 minutes of application time to effectively numb intact skin before intravenous catheter insertion. Timing is critical; applying EMLA only 15 minutes prior to venipuncture renders it useless.
The 2-4-6-8 Rule of Fasting
Anesthesia paralyzes the protective airway reflexes. If the stomach contains food or liquid, regurgitation leads directly to catastrophic pulmonary aspiration. However, prolonged fasting in young children causes hypoglycemia and severe dehydration. The solution is the 2-4-6-8 fasting algorithm, based entirely on gastric emptying rates:
| Intake Type | Preoperative Fasting Requirement | Rationale |
|---|---|---|
| Clear Liquids | Two hours | Water, clear apple juice, and Pedialyte empty from the stomach rapidly. |
| Breast Milk | Four hours | Higher fat content requires additional digestion time. |
| Infant Formula | Six hours | Curds and complex proteins take longer to break down than human milk. |
| Solid Foods | Eight hours | Full meals mandate maximum clearance time. |
Once the patient crosses the threshold into the operating room, the nursing priorities shift to rigid safety verification and the maintenance of physiological homeostasis.
The Surgical Time-Out
Wrong-site surgery is a "never event." The defense mechanism against this catastrophic error begins outside the OR: The primary surgeon must mark the pediatric surgical site with their initials before the patient enters the operating room.
Once inside, pediatric surgical time-outs require verbal confirmation of the patient's identity, the surgical site, and the specific procedure by the entire operating room team. If the scrub nurse, the anesthesiologist, or the circulating nurse spots a discrepancy, the procedure instantly halts.
The Thermodynamics of Hypothermia
Consider the geometry of an infant. Infants possess a disproportionately large body surface area to mass ratio compared to adults. In physics, heat is lost at the surface; a larger relative surface area means a faster rate of thermal transfer to the cold OR environment. Consequently, a large body surface area to mass ratio significantly increases an infant's susceptibility to perioperative hypothermia.
Hypothermia in a pediatric patient is not merely uncomfortable—it triggers coagulopathies, delays emergence from anesthesia, and increases oxygen consumption. To combat this, two primary interventions are engineered into the intraoperative workflow:
- Forced-air warming blankets are utilized intraoperatively to prevent hypothermia in pediatric surgical patients.
- Administering warmed intravenous fluids minimizes intraoperative heat loss in pediatric surgical patients by ensuring core temperature isn't eroded from the inside out.

Recovery from general anesthesia is a volatile physiological transition. The nursing imperative here is the rigorous defense of the airway and precise fluid resuscitation.
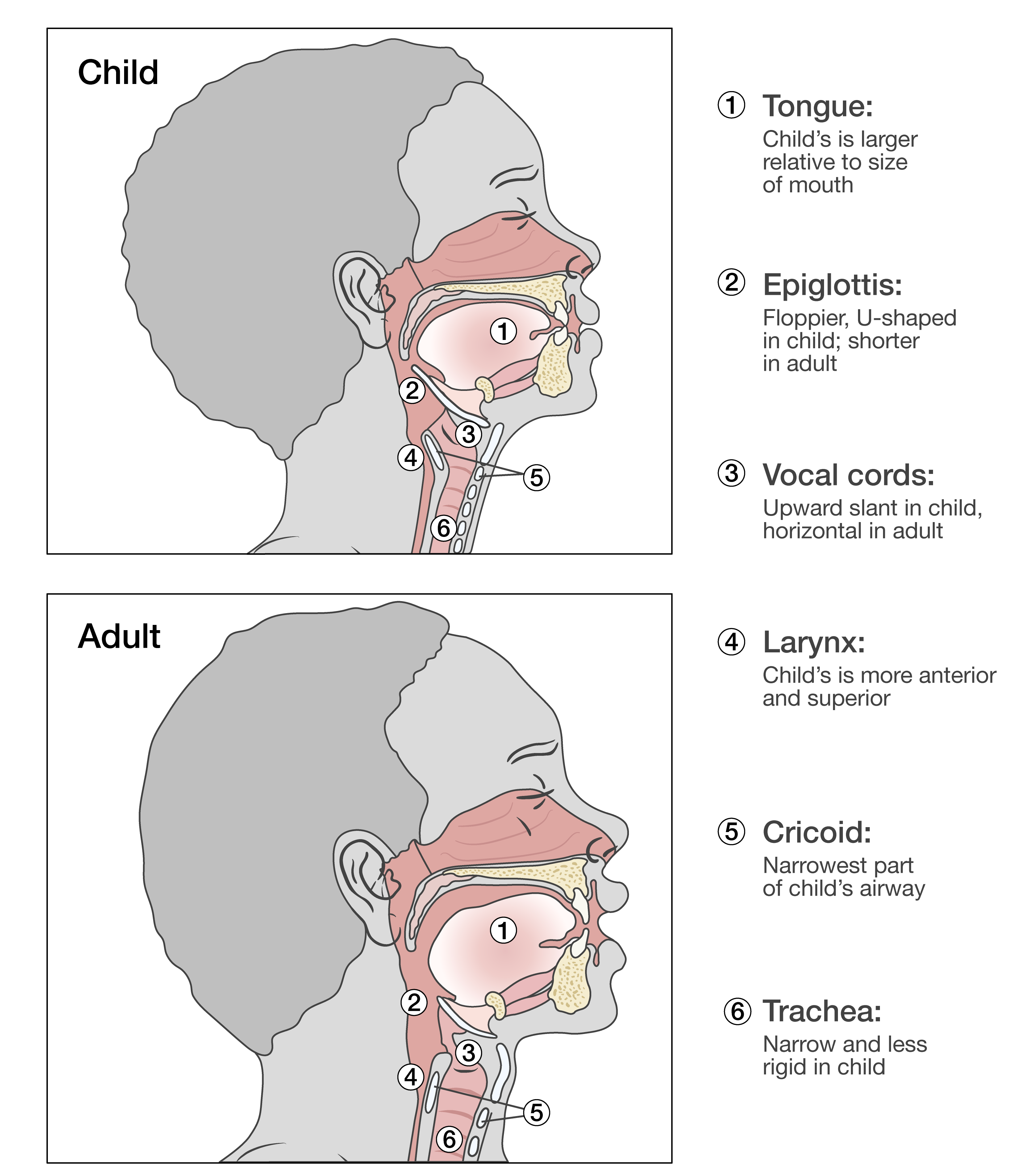
Defending the Airway
The pediatric airway is a funnel—wide at the top, narrow at the cricoid ring. A single millimeter of edema dramatically increases airflow resistance. Therefore, maintaining an open airway is the absolute first priority in the immediate postoperative management of a pediatric patient.
Two distinct airway emergencies dominate the PACU (Post-Anesthesia Care Unit):
- Stridor: A harsh, high-pitched respiratory sound. The presence of stridor in the immediate postoperative period indicates upper airway edema.
- Laryngospasm: A sudden, silent crisis. Laryngospasm is a life-threatening postoperative complication involving the sudden, involuntary spasm of the vocal cords, completely occluding airflow.
To protect the pediatric airway, two standard interventions are employed. First, the administration of humidified oxygen reduces airway mucosal irritation in postoperative pediatric patients, keeping secretions thin. Second, elevating the head of the bed postoperatively reduces the risk of aspiration in a pediatric patient recovering from anesthesia while simultaneously optimizing diaphragmatic excursion.
Postoperative Safety and Delirium
As the child metabolizes the anesthetic gases, they may wake up in a state of chaotic neurological misfiring. Postoperative emergence delirium manifests as acute confusion, thrashing, and extreme agitation in children awakening from general anesthesia.
Because a thrashing child is at high risk for injury, environmental controls are non-negotiable. Maintaining crib rails in the fully elevated position prevents postoperative falls in hospitalized pediatric patients.
Fluid Resuscitation: The 4-2-1 Rule
Children cannot regulate their fluid balance with the resilience of adults. They require meticulous maintenance fluid calculations based on their exact metabolic expenditure. Isotonic crystalloid solutions are the preferred maintenance intravenous fluids for pediatric surgical patients because they expand the intravascular volume without shifting fluid into the cells.
To calculate the exact hourly rate, we use an elegant, step-wise mathematical formula. The 4-2-1 rule is the standard formula used to calculate hourly maintenance intravenous fluid rates for pediatric patients.
The Mechanics of the 4-2-1 Rule:
- The 4-2-1 rule allocates 4 milliliters per kilogram per hour for the first 10 kilograms of a child's body weight.
- The 4-2-1 rule allocates 2 milliliters per kilogram per hour for the body weight between 11 and 20 kilograms.
- The 4-2-1 rule allocates 1 milliliter per kilogram per hour for every kilogram of body weight exceeding 20 kilograms.
Application: If a pediatric patient weighs 25 kg, the calculation is:
- First 10 kg: 10 kg × 4 mL = 40 mL/hr
- Next 10 kg: 10 kg × 2 mL = 20 mL/hr
- Remaining 5 kg: 5 kg × 1 mL = 5 mL/hr Total Maintenance Rate = 65 mL/hr.
Pain is an invisible variable. Because younger children lack the vocabulary to articulate their suffering, nurses must rely on validated, developmentally specific measurement instruments.
Validated Pain Scales
You cannot treat what you cannot measure. The SNLE demands precision in matching the pain scale to the patient's developmental age:
- Neonates: The CRIES scale assesses postoperative pain in neonates through evaluation of crying, oxygen requirement, vital signs, expression, and sleeplessness.
- Infants to Early School Age: The FLACC behavioral pain scale evaluates facial expression, leg movement, activity, cry, and consolability. The FLACC pain scale is validated for pain assessment in children aged two months to seven years.
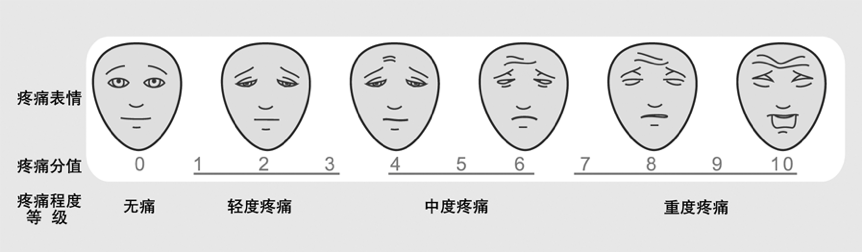
- Preschool and Up: The Wong-Baker FACES pain rating scale is validated for use in children aged three years and older, relying on the child pointing to a cartoon face that matches their internal state.
- Older Children: The numeric rating scale for pain assessment is generally appropriate for children aged eight years and older, as they can conceptualize numbers on a linear 0-to-10 scale.
Precision Pharmacology
A child’s liver and kidneys metabolize drugs at vastly different rates than an adult's. Therefore, pediatric medication dosages must be calculated strictly based on the child's exact body weight in kilograms. To prevent catastrophic decimal-point miscalculations, double-checking high-alert medications with a second registered nurse minimizes the risk of fatal dosing errors in pediatric care.
When pain strikes, we utilize an escalating ladder of interventions:
- Neonatal Non-Pharmacologic: The infant brain is wired to soothe through feeding mechanics. Non-nutritive sucking combined with oral sucrose administration reduces procedural pain in neonates by triggering endogenous opioid release.
- Mild to Moderate Pain:
- The standard pediatric dose of oral acetaminophen for postoperative pain management is 10 to 15 milligrams per kilogram per dose.
- The standard pediatric dose of oral ibuprofen for postoperative pain management is 5 to 10 milligrams per kilogram per dose.
- Severe Pain: Intravenous morphine is the preferred opioid analgesic for severe postoperative pain in pediatric patients.
Crucial Monitoring Warning: Opioids blunt the brainstem's drive to breathe. Therefore, continuous pulse oximetry monitoring is mandatory for all pediatric patients receiving opioid analgesics postoperatively.

The Absolute Contraindication
One specific analgesic carries a profound warning label. Codeine is strictly contraindicated in pediatric patients due to the high risk of life-threatening respiratory depression. Certain children possess genetic variations making them "ultra-rapid metabolizers" of codeine, causing their livers to convert the drug into massive, fatal doses of morphine in the bloodstream. Administering codeine to a child is an indefensible error.