Co-occurring Conditions
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
Imagine observing two intersecting wave crests in a pond. When the wave crests meet, they do not simply coexist side by side; they amplify each other, creating a disturbance far greater than the sum of their individual amplitudes. In the human mind, developmental and learning exceptionalities interact in precisely the same way. The intersection of different neurological, behavioral, or cognitive profiles does not produce simple addition; it creates an entirely new topography of learning.
This is the realm of comorbidity, which refers to the simultaneous presence of two or more disabilities or conditions in a single individual. As a special educator, you will rarely encounter a student whose mind fits neatly into a single diagnostic box. The brain is an interconnected network, and a structural or chemical variance in one area often cascades into others. To teach effectively, you must understand not just the isolated conditions, but the complex chemistry of how they interact, mask one another, and ultimately dictate a student's educational needs.
When we observe a student struggling, we naturally look for a root cause. However, human cognition is rarely that cooperative. Rather than experiencing two distinct sets of challenges, co-occurring conditions often create an interactive effect that exponentially compounds a student's overall learning difficulties.
If a student has a learning disability in reading (dyslexia) and also experiences an attention disorder, the reading deficit makes focusing highly fatiguing, while the attention deficit ensures the student misses the foundational phonics instruction necessary to fix the reading gap. The result is a magnified hurdle.
The Illusion of the Primary Diagnosis
One of the greatest traps in special education is the assumption that the most visible behavior is the only problem. Because some conditions are loud and disruptive, while others are silent and internal, the prominent symptoms of one primary disability can mask the symptoms of a secondary co-occurring condition.
Diagnostic Overshadowing Diagnostic overshadowing occurs when a student's observed behaviors are entirely attributed to a known disability while a secondary condition goes unrecognized.
Imagine a student diagnosed with Attention-Deficit/Hyperactivity Disorder (ADHD) who is constantly acting out during independent reading time. It is dangerously easy to attribute this defiance solely to impulsivity and a lack of focus stemming from ADHD. But what if the student is acting out because they cannot decode the words on the page? If the ADHD overshadows a hidden Specific Learning Disability (SLD), the true source of the student's suffering goes unaddressed. You might implement an elaborate behavioral token economy, but no amount of stickers will teach a child how to read.
Certain conditions share deep neurological real estate or cascading developmental pathways, meaning they cluster together with remarkable statistical predictability. Recognizing these patterns allows you to anticipate challenges rather than merely reacting to them.
1. ADHD and the Learning-Behavior Nexus
ADHD is perhaps the most frequent traveler in the realm of comorbidity.
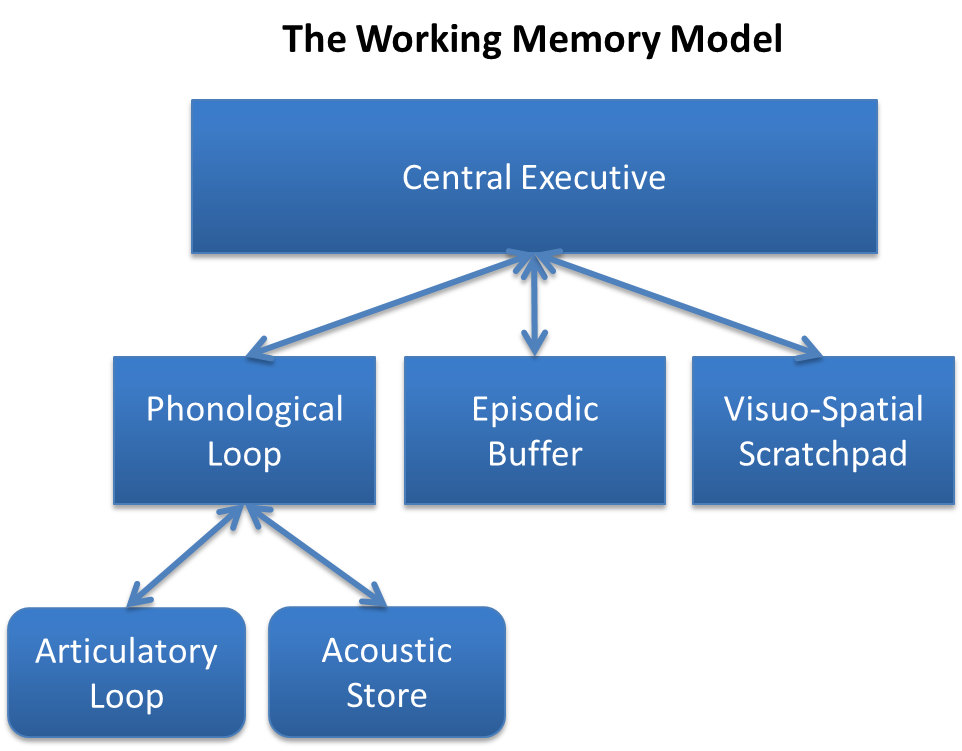
- ADHD and Specific Learning Disabilities (SLD): Attention-Deficit/Hyperactivity Disorder co-occurs with Specific Learning Disabilities in approximately 30 to 50 percent of cases. This is a staggering overlap. Why? Because executive functioning deficits are common underlying traits in both ADHD and Specific Learning Disabilities. Both conditions struggle with the brain's "managerial" tasks: working memory, organization, and processing speed.
- ADHD and Oppositional Defiant Disorder (ODD): The impulsivity and emotional dysregulation inherent in ADHD can easily manifest as defiance. Consequently, Oppositional Defiant Disorder frequently co-occurs with Attention-Deficit/Hyperactivity Disorder.
2. The Tourette Syndrome Triad
Tourette Syndrome is a neurological disorder characterized by involuntary tics. However, the tics are rarely isolated. The basal ganglia circuitry involved in Tourette Syndrome is intimately connected to impulse control and anxiety pathways.
- Tourette Syndrome frequently co-occurs with Attention-Deficit/Hyperactivity Disorder.
- Tourette Syndrome frequently co-occurs with Obsessive-Compulsive Disorder (OCD).
3. Autism Spectrum Disorder (ASD) Clusters
The neurodivergent architecture of Autism Spectrum Disorder spans a vast range of presentations, but it frequently runs parallel to two distinct conditions:
- ASD and Intellectual Disability (ID): Autism Spectrum Disorder frequently co-occurs with Intellectual Disability, requiring instruction that targets both adaptive communication skills and foundational cognitive development.
- ASD and Anxiety: Navigating a world with profound sensory sensitivities and rigid expectations is inherently stressful. Therefore, anxiety disorders frequently co-occur with Autism Spectrum Disorder. A meltdown in the classroom is rarely just "behavior"—it is often a severe anxiety response triggered by sensory or routine disruptions.
4. Language, Learning, and the Emotional Cascade
- Speech/Language and Reading: Language is the foundation of literacy. Consequently, speech and language impairments frequently co-occur with reading disabilities such as dyslexia. A child who struggles to process the sounds of spoken language will almost inevitably struggle to map those sounds onto written letters.
- SLD and Emotional/Behavioral Disorders (EBD): Emotional and Behavioral Disorders frequently co-occur with Specific Learning Disabilities. This is often a matter of cause and effect. Secondary emotional or behavioral issues can develop as a direct result of the chronic frustration associated with an untreated Specific Learning Disability. Imagine sitting in a room where everyone is speaking a language you do not understand, and you are punished for failing to answer questions. Defiance or depression becomes a logical defense mechanism.
5. Physical and Medical Co-occurrence
- Cerebral Palsy and Epilepsy: Cerebral Palsy arises from damage or abnormal development in the parts of the brain that control movement. Because this is a structural neurological issue, the brain's electrical activity is often impacted as well. Thus, epilepsy is a common co-occurring medical condition in students diagnosed with Cerebral Palsy.
| Primary Condition | Most Common Co-Occurring Conditions | Shared Underlying Mechanisms / Triggers |
|---|---|---|
| ADHD | Specific Learning Disability (SLD), ODD | Executive functioning deficits, impulsivity |
| Autism (ASD) | Intellectual Disability (ID), Anxiety | Sensory processing, cognitive rigidity |
| Tourette Syndrome | ADHD, OCD | Basal ganglia neurological circuitry |
| SLD (e.g., Dyslexia) | Speech/Language Impairment, EBD | Phonological processing, chronic academic frustration |
Because of the compounding nature of these conditions, a student with co-occurring conditions may exhibit a highly uneven profile of academic strengths and weaknesses. A student with ASD and an anxiety disorder might possess an exceptional, encyclopedic memory for historical dates but become completely non-verbal when asked to work in a peer group.
This unevenness requires nuance, particularly when addressing the massive overlap between ADHD and SLD.
The Limitations of Single-Pronged Interventions
It is a common misconception among parents and novice educators that if a student is medicated for ADHD, their academic struggles will vanish. This is physiologically false. Pharmacological treatments for ADHD do not cure or resolve co-occurring Specific Learning Disabilities. Medication may widen the student's window of attention, but if the student lacks the phonetic decoding skills to read, they will simply be paying closer attention to a page they still cannot understand.
Therefore, educators must implement explicit academic instruction alongside behavioral interventions for students with comorbid ADHD and Specific Learning Disabilities. Interventions for a student with co-occurring ADHD and learning disabilities must target both behavioral regulation (like self-monitoring checklists or structured breaks) and academic skill deficits (like direct, sequential phonics instruction).
Because diagnostic overshadowing is so dangerous, the law leaves no room for guesswork. Under the Individuals with Disabilities Education Act (IDEA), evaluators must assess a student in all areas related to any suspected disability. If a student is referred for behavioral issues, but a learning disability is even remotely suspected as a contributing factor, the school district is legally obligated to assess their academic and cognitive functioning alongside their behavior.
The "Multiple Disabilities" Eligibility Category
When a student presents with multiple, severe interacting conditions, how does special education classify them to ensure they receive funding and support?
The Individuals with Disabilities Education Act (IDEA) includes a specific eligibility category named Multiple Disabilities.
IDEA Definition: The IDEA defines Multiple Disabilities as concomitant impairments (such as intellectual disability-blindness, or intellectual disability-orthopedic impairment) that cause severe educational needs.
The crux of this legal definition hinges on the interactive effect we discussed earlier. The needs caused by these combined conditions are so severe that a student classified with Multiple Disabilities under IDEA cannot be accommodated in a special education program designed solely for one of the student's impairments.
For example, a student with severe Intellectual Disability and a severe Orthopedic Impairment cannot simply be placed in a standard life-skills room without profound physical adaptations, nor can they be placed in a purely physical-rehabilitation setting that ignores their cognitive development. Students with multiple diagnoses require educational programming that explicitly addresses the combined effects of all their conditions simultaneously.
Note on Deaf-blindness: There is one specific exception to this grouping rule. The Individuals with Disabilities Education Act categorizes Deaf-blindness as a distinct eligibility category rather than grouping it under Multiple Disabilities. The loss of both primary distance senses (vision and hearing) creates such unique communication and developmental demands that it necessitates its own specialized classification and expertise.
No single teacher possesses the total depth of expertise required to independently design a program for a student with severe comorbid conditions. You might be a master of explicit reading instruction for SLD, but you are not a licensed speech-language pathologist, nor an occupational therapist, nor a child psychiatrist.
For this reason, multidisciplinary collaboration is strictly necessary to design effective Individualized Education Programs (IEPs) for students with co-occurring conditions.
Creating an IEP for a student with Tourette Syndrome, OCD, and ADHD requires the school psychologist to help navigate anxiety triggers, the special education teacher to implement executive functioning scaffolds, the general education teacher to provide flexible seating, and the parents to report on medication efficacy.
As an educator, your role is not to cure these conditions. Your role is to serve as the orchestrator of this multidisciplinary team, ensuring that you view the student not as a collection of isolated broken parts, but as a complex, whole human being whose unique mind requires an equally unique, multi-layered approach to teaching.