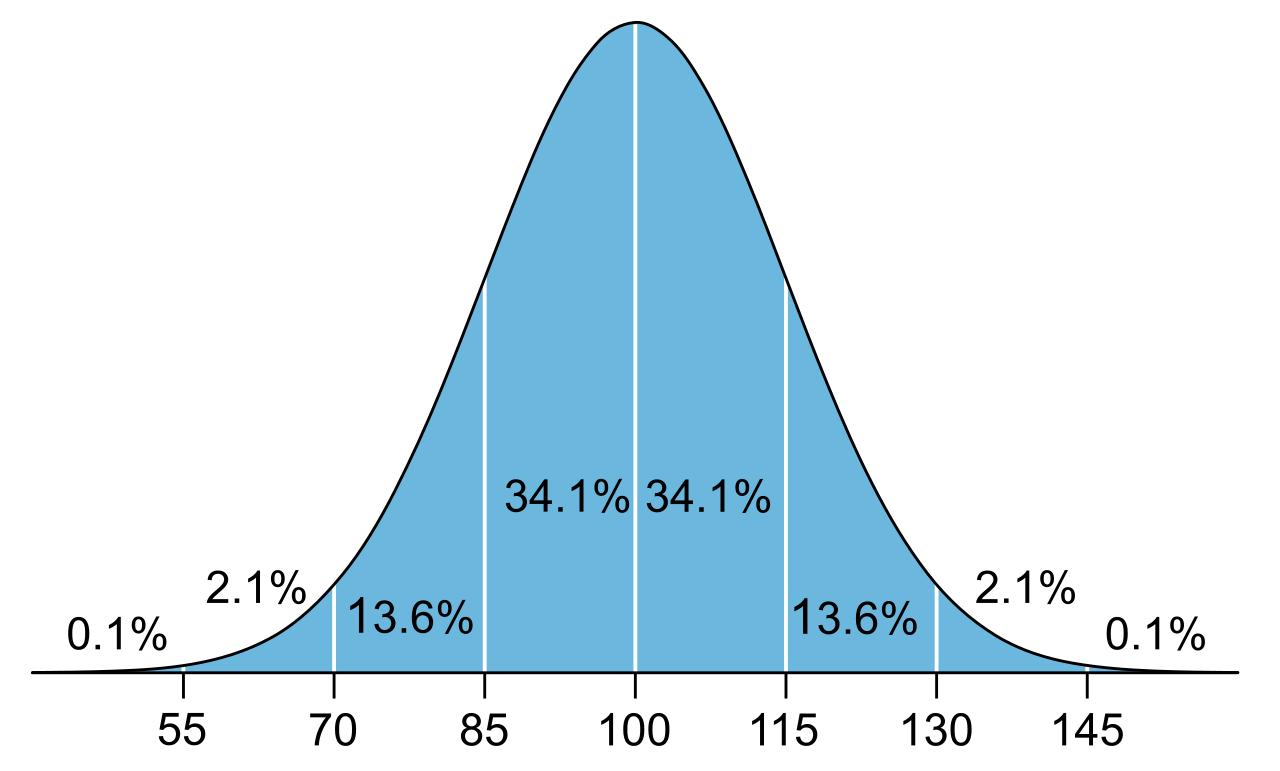
Historically, the educational system diagnosed specific learning disabilities much like a civil engineer waiting for a bridge to buckle before determining the steel was weak. This older paradigm relied on the severe discrepancy model, a diagnostic standard that required a significant statistical gap between a student’s intelligence quotient (IQ) score and their actual academic achievement level. By its very design, this was a "wait-to-fail" system; it mandated profound, measurable academic failure before a student could unlock targeted support.
A standard Intelligence Quotient (IQ) distribution curve. The severe discrepancy model historically required a statistically significant gap between this expected IQ baseline and a student's actual academic achievement to diagnose a learning disability.
Today, special education operates on a fundamentally different premise: proactive structural reinforcement. Rather than waiting for collapse, we apply standardized stress tests early, map the exact coordinates of academic and behavioral weaknesses, and reinforce those areas using instructional methodologies proven by scientific rigor.
This guide explores the architecture of that proactive system—how we select validated tools, how we deploy them, and how we measure their impact.
If you were diagnosed with a severe infection, you would expect your physician to prescribe a medication proven to eliminate that specific bacteria, not an experimental herb they read about in a lifestyle magazine. Special education demands the exact same rigor.
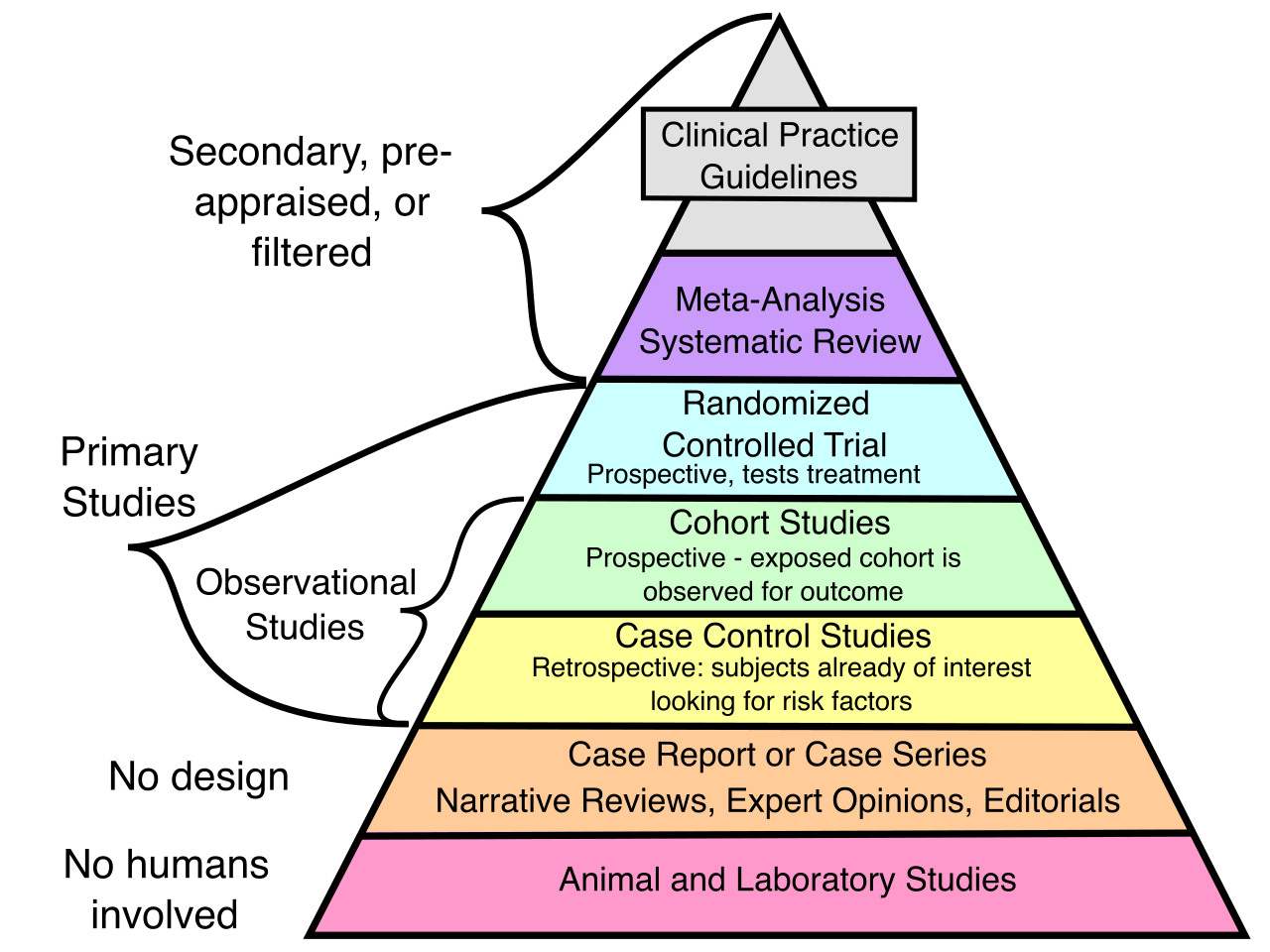
Evidence-based practices (EBPs) are instructional techniques supported by rigorous scientific research demonstrating positive student outcomes. They are not fads, and they are not guesswork; they are pedagogical tools that have survived the crucible of peer-reviewed statistical analysis.
Evidence-based practices in education require the same levels of rigorous scientific validation and hierarchical research design used to determine efficacy in evidence-based medicine.
To help educators cut through the noise of educational marketing, the federal government maintains the What Works Clearinghouse. This is a federal database that rigorously reviews and rates the effectiveness of specific educational interventions, serving as an authoritative index of what actually works in the classroom.
Identifying a brilliant, research-backed intervention is only half the battle. The other half is execution.
In research, an intervention’s success is entirely dependent on its precise administration. Intervention fidelity is the act of delivering an instructional program exactly as the original developers intended. High intervention fidelity requires strict adherence to the dosage (how much time per session) and schedule (how many days per week) specified by the original intervention designers.
The Golden Rule of Fidelity:
Modifying a research-based intervention before gathering baseline data compromises the established validity of the intervention.
If an educator implements a Tier 2 reading program designed for 45 minutes a day, but truncates it to 20 minutes to fit a scheduling quirk, the intervention has been fundamentally compromised. If the student fails to progress, the educator cannot definitively say the student has a learning deficit; the failure might simply be a byproduct of a diluted, low-fidelity intervention.
To deploy these evidence-based practices systematically, modern schools rely on tiered frameworks. The broadest of these is the Multi-Tiered System of Supports (MTSS). Think of MTSS as the overarching ecosystem of a school; it is a comprehensive educational framework encompassing both academic and behavioral student interventions.
Nested within MTSS is Response to Intervention (RTI). RTI is a preventative academic framework designed to identify and support struggling students early in the educational process.
The brilliance of RTI lies in its paradigm shift. The Response to Intervention framework serves as an alternative to the severe discrepancy model for identifying specific learning disabilities. In fact, IDEA legally allows schools to use a student's response to scientific interventions to identify specific learning disabilities.
Why is this important? Because the Response to Intervention framework is explicitly designed to prevent the over-identification of students with specific learning disabilities. By providing high-quality, scientifically backed instruction before evaluating for special education, RTI allows educators to rule out "poor instruction" as the primary cause of a student's academic failure.
The Response to Intervention framework typically consists of three distinct tiers of increasing instructional intensity. Before students are placed into tiers, the school utilizes universal screening—the systematic assessment of all general education students to identify individuals at risk for academic or behavioral difficulties. Universal screening in a Response to Intervention framework typically occurs two to three times per academic school year.
Once screening data is collected, targeted interventions must directly align with the specific academic deficits identified. If universal screening reveals a deficit in phonemic segmentation, the student must receive an intervention targeting phonemic segmentation, not broad reading comprehension.
Tier Level
Core Function & Environment
Target Population
Tier 1
Involves high-quality core instruction provided to all students in the general education classroom.
Statistically designed to meet the academic needs of approximately 80% of the student population.
Tier 2
Provides targeted small-group interventions for students who do not make adequate progress in Tier 1.
Statistically designed to support approximately 15% of the student population.
Tier 3
Provides the most intensive individualized academic interventions for students who do not respond to Tier 2 supports.
Statistically designed to support approximately 5% of the student population.
If a student receives high-fidelity, evidence-based instruction across all three tiers and still shows insufficient growth, the system has effectively ruled out lack of instruction as the root cause. At this juncture, students who fail to respond adequately to intensive Tier 3 interventions may be referred for a comprehensive special education evaluation.
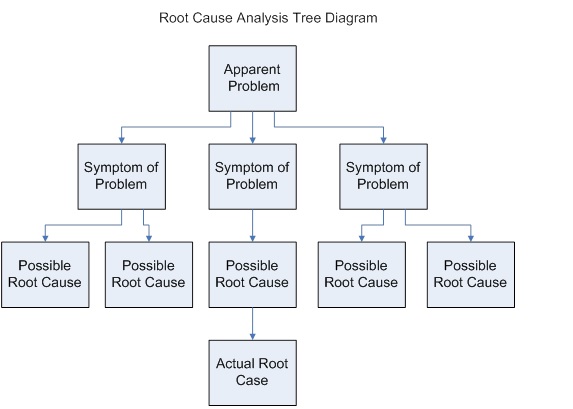
The RTI framework functions as a practical root cause analysis, systematically ruling out poor instruction as the primary reason for academic failure before ever considering special education referrals.
How do we know when a student requires movement between these tiers? We rely on data-based decision making, which involves using objective student assessment data to guide instructional adjustments and intervention selection.
The engine driving this decision-making process is progress monitoring—the frequent and ongoing assessment of a student's academic performance to evaluate the effectiveness of a specific intervention. If universal screening is the yearly physical exam, progress monitoring is the heart monitor worn during a stress test.
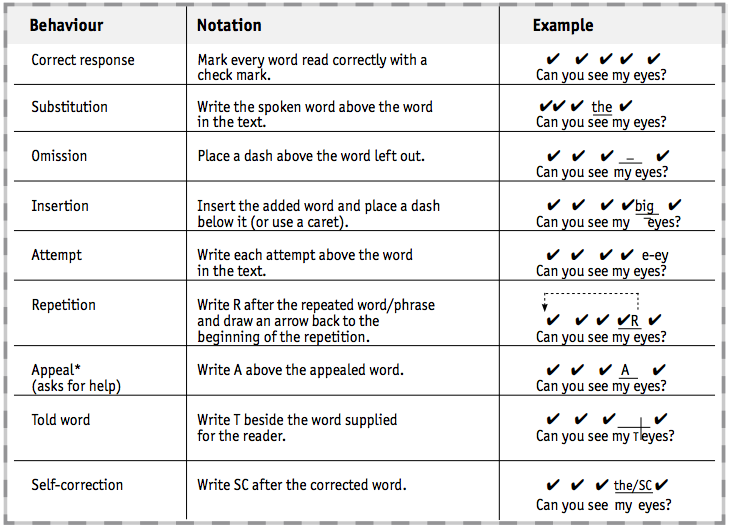
To execute progress monitoring efficiently, educators use curriculum-based measurement (CBM). A CBM is a standardized assessment tool frequently used for academic progress monitoring within a Response to Intervention framework. These are brief, highly reliable probes (like a one-minute oral reading fluency check or a two-minute math computation sheet) that can be administered weekly or bi-weekly.
Curriculum-based measurements often utilize standardized scoring codes, such as these running record symbols, to systematically track a student's oral reading fluency and specific error patterns.
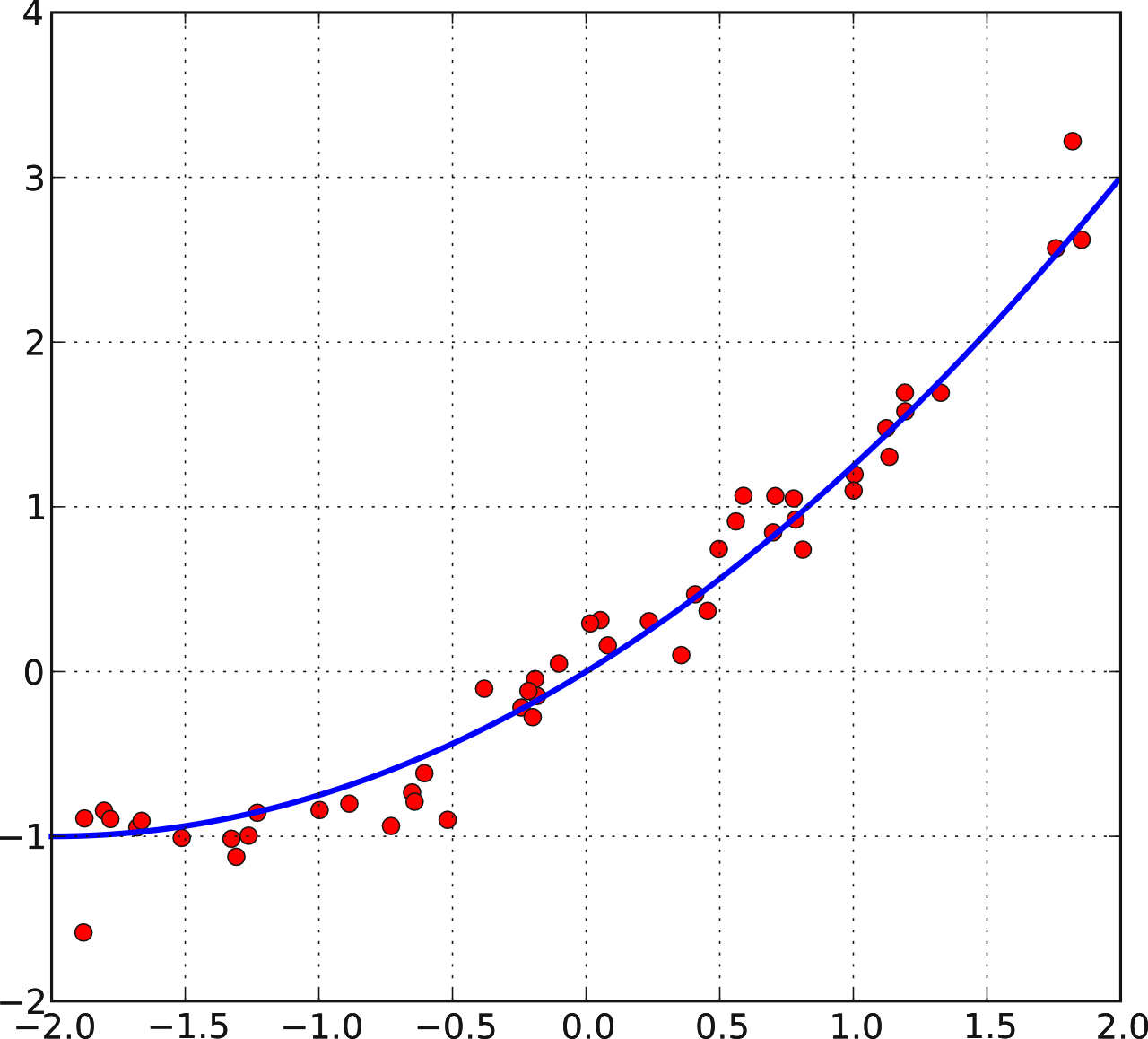
When plotted on a graph, these CBM data points form a trendline. Ultimately, a student's rate of growth on a curriculum-based measurement dictates whether an academic intervention should be maintained or altered.
By plotting curriculum-based measurement data points over time, educators can calculate a trendline (blue) to evaluate whether a student's current rate of growth is sufficient to intercept grade-level expectations.
If the rate of growth is steep enough to intercept grade-level expectations, the intervention is maintained. If the rate of growth is flat, the intervention must be altered—either by increasing the dosage, tightening the fidelity, or selecting a new evidence-based practice entirely. In this way, special education becomes less of an administrative label and more of a dynamic, scientific pursuit of what uniquely works for the mind of the individual student.