Long-term insurance and long-term case planning (individual and group)
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
A fundamental principle in physics is that systems tend toward entropy—things break down. The human body is no exception. In financial planning, the breakdown of the physical mind or body presents a singular, catastrophic risk that can dismantle decades of compounded wealth in a matter of months. When you sit across from a client who has spent a lifetime accumulating a pristine portfolio, the most statistically probable threat to that portfolio is not a market crash or an estate tax change; it is the cost of long-term custodial care. To protect against this, we must understand exactly how the machinery of long-term care (LTC) funding works, from the precise biological triggers that unlock capital, to the mathematical structure of the insurance contracts, down to the rigid federal statutes governing public aid.

Insurance is simply a contract that transfers risk, but a contract must have perfectly defined boundaries. We cannot use subjective terms like "getting old" or "feeling frail." The industry and the tax code have synchronized around a highly specific set of biological and cognitive thresholds that trigger policy benefits.
To receive benefits from a qualified long-term care insurance policy, the insured must meet one of two distinct triggers.
The Physical Trigger: Activities of Daily Living (ADLs)
The first trigger is strictly physical. The insured must be certified by a licensed healthcare practitioner as unable to perform at least two of the six Activities of Daily Living (ADLs) without substantial assistance.
You must commit these six ADLs to memory, not just for the exam, but because they are the universal language of eldercare:
- Eating: The ability to feed oneself.
- Bathing: The ability to wash oneself in a tub, shower, or by sponge bath.
- Dressing: The ability to put on and take off all necessary items of clothing.
- Transferring: The ability to move into or out of a bed, chair, or wheelchair.
- Toileting: The ability to get to and from the toilet and perform associated personal hygiene.
- Continence: The ability to maintain control of bowel and bladder function.
Crucial Timing Constraint: The inability to perform these ADLs is not a short-term pass for a twisted ankle. The impairment must be expected to last for at least 90 days to trigger qualified long-term care insurance benefits.
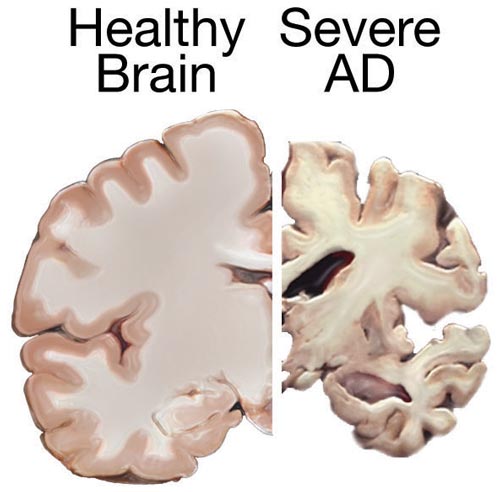
The Cognitive Trigger
The human body can be perfectly healthy while the brain fails. Because of this, severe cognitive impairment requiring substantial supervision triggers qualified long-term care insurance benefits regardless of the insured's physical ability to perform Activities of Daily Living. If an Alzheimer's patient can physically bathe, dress, and eat, but will wander into traffic or leave a stove burner on, they qualify for benefits under the cognitive impairment trigger.
Before a client will buy private insurance, they often assume the government will simply take care of them. You must ruthlessly dismantle the confusion between Medicare and Medicaid. They are profoundly different systems with different goals.
The Medicare Misconception
Medicare does not cover long-term custodial care services. Period. Custodial care—help with the ADLs we just defined—is not considered medical treatment; it is personal care.
Medicare is designed to acute care and rehabilitation. It will cover skilled nursing care, but under highly restricted, temporary conditions:
- Prerequisite: Medicare skilled nursing care coverage requires a preceding qualifying inpatient hospital stay of at least three consecutive days. (Observation status does not count).
- Duration Limit: If the client qualifies, Medicare covers a maximum of 100 days of skilled nursing care per benefit period.
After 100 days, or the moment the care transitions from "skilled rehabilitation" to "custodial," Medicare ceases to pay.
The Medicaid Reality
If Medicare is for short-term rehabilitation, Medicaid is a joint federal and state program that serves as the primary payer of custodial long-term care costs for individuals with limited financial resources.
Medicaid is essentially a welfare program. To qualify, a client must be impoverished, which introduces the necessity of Medicaid planning. The government anticipates that wealthy individuals might simply give all their money to their children on Monday to qualify for taxpayer-funded care on Tuesday. To prevent this, Medicaid imposes a 60-month look-back period on all asset transfers to evaluate an applicant's eligibility.
If you transfer assets to your heirs—or anyone else—for less than fair market value during this 60-month look-back period, it generates a penalty period of ineligibility for Medicaid long-term care benefits. The math here is simple but brutal: the state takes the dollar amount of the uncompensated transfer and divides it by the average monthly cost of care in the state to determine exactly how many months the applicant will be denied benefits.
However, the government does not want to force a healthy spouse to live under a bridge just because their partner developed dementia. Medicaid spousal impoverishment rules allow a community spouse (the healthy spouse staying at home) to retain a legally specified amount of combined marital assets while the institutionalized spouse receives Medicaid long-term care benefits. Furthermore, to prevent sudden homelessness, a primary residence is generally excluded from countable assets for Medicaid long-term care eligibility up to a federally specified home equity limit.
If a client wants to avoid Medicaid impoverishment and dictate the quality of their own care, they must self-fund or transfer the risk to an insurance company. There are two primary architectural frameworks for this transfer.
Traditional Standalone Long-Term Care Insurance
Historically, LTC insurance was sold like auto or homeowners insurance. You pay an annual premium, and if you need care, the policy pays out.
- The Catch: Traditional standalone long-term care insurance policies operate on a use-it-or-lose-it basis. Furthermore, they provide no return of premium or residual value to beneficiaries if the policyholder dies without needing care. If a client pays premiums for 25 years and dies peacefully in their sleep, all that capital is gone.
- The Rate Risk: Traditional standalone policies typically allow the insurance company to increase premium rates for an entire class of policyholders in a specific state. Over the last two decades, actuaries severely underestimated how long people would live and how much care would cost, leading to massive, painful premium hikes for existing policyholders.
Hybrid Life/LTC Policies
To solve the psychological hurdle of "use-it-or-lose-it" and the financial terror of rising premiums, the industry engineered the hybrid policy.
Hybrid long-term care policies link long-term care coverage with a permanent life insurance policy or a fixed annuity. By fusing these instruments, the mechanics completely change:
- The Guarantee: Hybrid long-term care policies guarantee a death benefit or annuity payout to beneficiaries if the insured does not exhaust the long-term care benefits. If you need care, it pays for care. If you die without needing care, your heirs get a tax-free life insurance payout. You are guaranteed a return of capital in one form or another.
- Price Stability: Because these policies are often funded with a large single premium or a fixed payment schedule over a short duration, hybrid long-term care policies generally feature guaranteed premiums that cannot be increased by the insurance company over the life of the policy.
Note: You can also attach a long-term care rider on a life insurance policy [which] accelerates the life insurance death benefit to pay for the insured's qualified long-term care expenses. It achieves a similar result: burning down the death benefit while alive to fund care.
| Feature | Traditional Standalone LTC | Hybrid Life/LTC Policy |
|---|---|---|
| Residual Value | None (Use-it-or-lose-it) | Guaranteed death benefit or annuity payout |
| Premium Stability | Subject to class-based rate increases | Guaranteed; cannot be increased |
| Primary Objection | Sunk cost if care is never needed | Requires significant upfront capital |
When constructing a policy, we have specific levers we can pull to adjust the cost and the coverage.
The Elimination Period
Just as a health insurance policy has a deductible measured in dollars, the elimination period on a long-term care insurance policy functions as a time-based deductible. It is the number of days the client must pay for care out-of-pocket before the insurance company cuts the first check. By shifting more of the initial risk to the client, selecting a longer elimination period on a long-term care insurance policy decreases the policy's premium cost.
Inflation Protection
A daily benefit of $250 might cover a nice facility today, but in twenty years, it will cover very little. Inflation riders are mandatory considerations.
- Simple inflation protection riders increase the long-term care benefit amount by a fixed percentage of the original baseline benefit amount. (e.g., A 5% simple rider on a $100 daily benefit adds $5 every single year, forever).
- Compound inflation protection riders increase the long-term care benefit amount by a fixed percentage of the previous year's benefit amount. Because the growth compounds, this is vastly superior for a younger client, though much more expensive.
The Shared Care Rider
Couples face a unique risk: one spouse might suffer a severe, decade-long illness that completely exhausts their individual policy limits, while the other spouse's policy sits untouched. A shared care rider on a long-term care policy allows spouses to pool their combined benefits and utilize the other spouse's benefit pool if one exhausts their own coverage. It treats the marital unit's risk as a single, connected reservoir.
Do not overlook the workplace as a source of risk management. Employers often offer group LTC policies, which possess two massive advantages for certain clients:
- Underwriting Bypass: Group long-term care insurance policies offered through employers are often guaranteed issue up to certain coverage limits without requiring individual medical underwriting. This is a golden opportunity for clients with pre-existing conditions who would otherwise be uninsurable in the private retail market.
- Portability: Unlike many group health insurance policies that terminate or become prohibitively expensive via COBRA when you leave a job, group long-term care insurance policies are generally portable upon separation from service. The client can keep paying the premium directly to the insurer and retain the coverage into retirement.
The tax code incentivizes Americans to purchase private LTC insurance so the burden does not fall on Medicaid.
Tax Treatment of Premiums and Benefits
From an income perspective, the mechanics are highly favorable:
- Benefits received from a qualified long-term care insurance policy are generally excluded from the gross income of the recipient. Just like standard health insurance payouts, they are tax-free.
- Premiums paid for a qualified long-term care insurance policy are treated as deductible medical expenses subject to the taxpayer's adjusted gross income floor.
- However, the IRS does not allow unlimited deductions. The maximum deductible premium amount allowed for a qualified long-term care insurance policy is determined by the attained age of the insured at the end of the tax year. The older you get, the higher the allowable deduction limit.
State Long-Term Care Partnership Programs
Finally, we arrive at one of the most elegant intersections of private planning and public policy.
What happens if a client buys a moderate LTC policy (say, $300,000 in total benefits), suffers a catastrophic illness, and exhausts the entire policy? Historically, they would then have to spend down all their remaining personal assets to Medicaid poverty levels to get government help.
To encourage middle-class citizens to buy at least some insurance, State Long-Term Care Partnership programs allow individuals who exhaust qualified long-term care insurance benefits to protect a matching dollar amount of personal assets from Medicaid spend-down requirements.
If a client purchases a Partnership-qualified policy that pays out $300,000 in benefits, and those benefits are eventually exhausted, the state will allow that client to keep $300,000 in countable assets above and beyond the standard Medicaid impoverishment limits, and still qualify for Medicaid coverage. It is a dollar-for-dollar asset protection shield. This allows a planner to design a policy that perfectly protects a client's desired legacy without needing to buy a massively expensive unlimited lifetime policy.
Understanding these frameworks is not simply about passing the CFP Certification exam; it is about recognizing the precise physics of a client's risk exposure. By mastering the biological triggers, the tax rules, the hybrid engineering, and the Medicaid safety nets, you become the architect of a perimeter that ensures your client's wealth outlives their body's eventual breakdown.