Co-occurring Conditions
Not sure you’re ready?
Take the ~3-minute readiness diagnostic and see where you stand.
A student’s cognitive and behavioral profile is rarely a single, isolated variable; it is a dynamic system of interacting forces. If you pluck one string on a guitar, the entire instrument resonates. In the classroom, when a student presents with a disability, we are rarely looking at a siloed impairment. We are looking at a complex ecology of neurology, behavior, and environment. Comorbidity refers to the simultaneous presence of two or more chronic diseases or conditions in a single individual. For the aspiring special education teacher, understanding comorbidity is not merely an exercise in vocabulary—it is the lens through which you will decode the most perplexing challenges your students face.
When a student has multiple conditions, their difficulties do not simply add together; they multiply. Co-occurring disabilities interact to create educational needs greater than the sum of the individual conditions.
Imagine a student with a specific learning disability in reading. Now, imagine that same student also has poor executive functioning. The reading deficit requires deliberate, sustained cognitive effort, but the executive functioning deficit makes sustaining that effort nearly impossible. The interaction creates a uniquely formidable barrier.
The Danger of Diagnostic Overshadowing
When we see a prominent, highly visible disability—like a severe behavioral disorder or Autism Spectrum Disorder—it often commands our full attention. This cognitive bias leads to a phenomenon known as diagnostic overshadowing.
Diagnostic Overshadowing occurs when an evaluator attributes a student's symptoms entirely to an existing primary diagnosis.
Because the most obvious disability acts like a glaring spotlight, it blinds the observer to everything sitting in the shadows. Consequently, diagnostic overshadowing often prevents the identification of secondary or co-occurring disabilities in students. If a student with Autism is struggling to read, an evaluator might wrongly assume the struggle is simply a manifestation of the Autism, completely missing an underlying, highly treatable learning disability.
This requires rigorous vigilance from the evaluation team. Multidisciplinary team evaluations are strictly required to accurately identify the presence of overlapping disabilities. You cannot rely on a single perspective; school psychologists, speech-language pathologists, occupational therapists, and special educators must triangulate their findings to see the whole child.
The Individuals with Disabilities Education Act (IDEA) recognizes that some combinations of disabilities require highly specialized frameworks.
The "Multiple Disabilities" Category
Under the Individuals with Disabilities Education Act, Multiple Disabilities is a specific, distinct disability category. However, a student does not receive this classification simply for having two conditions like ADHD and a mild learning disability.
The Multiple Disabilities category classification requires the simultaneous presence of impairments that cause severe educational needs. Crucially, students classified under Multiple Disabilities have educational needs that cannot be accommodated in a special education program solely for one of the impairments. For example, a student with severe intellectual disability and orthopedic impairment requires an environment engineered for both; treating one while ignoring the other will result in systemic educational failure.
Crucial IDEA Distinction: The Multiple Disabilities category does not include deaf-blindness under the Individuals with Disabilities Education Act. Because the intersection of deafness and blindness creates such unique, intense communication and developmental needs, deaf-blindness is treated as its own independent disability category under the Individuals with Disabilities Education Act.
The Comprehensive IEP Guarantee
Regardless of the legal label placed on the front page of the document, an Individualized Education Program must comprehensively address all of a student's disability-related needs regardless of the primary disability label. If a student’s primary label is Emotional Disturbance, but they also have a speech impairment, the IEP must contain goals and services for the speech impairment.
Because of this, interventions for multiple disabilities necessitate close coordination among special educators and related service providers. The occupational therapist, the classroom teacher, and the behavior analyst cannot operate in silos; their interventions must interlock.
To succeed in the classroom (and on your licensure exams), you must recognize the most statistically probable intersections of disabilities. Neurology rarely confines itself to neat, singular boxes.
The ADHD Nexus
Attention Deficit Hyperactivity Disorder (ADHD) is the great "co-traveler" of the special education world. It frequently shares neurological real estate with a variety of other conditions.
- ADHD and Learning Disabilities: Approximately one-third to one-half of children with Attention Deficit Hyperactivity Disorder also have a Specific Learning Disability. This is a critical demographic. Executive functioning deficits inherent in Attention Deficit Hyperactivity Disorder exacerbate the academic challenges of a Specific Learning Disability. For example, working memory deficits associated with Attention Deficit Hyperactivity Disorder compound the decoding difficulties seen in dyslexia. The student cannot hold the sound of the first syllable in their mind long enough to blend it with the second syllable. Therefore, accommodations for a student with both a Specific Learning Disability and Attention Deficit Hyperactivity Disorder must simultaneously support academic skill deficits and self-regulation. Providing graphic organizers (skill support) while ignoring the need for frequent movement breaks (self-regulation) will fail.
- ADHD and Behavioral/Mood Disorders: Oppositional Defiant Disorder frequently co-occurs with Attention Deficit Hyperactivity Disorder. The impulsivity of ADHD often fuels the reactive defiance of ODD. Furthermore, bipolar disorder has a high rate of comorbidity with Attention Deficit Hyperactivity Disorder in children and adolescents, presenting a complex web of mood dysregulation and attention deficits.
- ADHD and ASD: It is highly common to see overlapping traits; Attention Deficit Hyperactivity Disorder frequently co-occurs with Autism Spectrum Disorder.
- ADHD and Tourette Syndrome: Individuals with Tourette syndrome frequently present with co-occurring Attention Deficit Hyperactivity Disorder.
Specific Learning Disability (SLD) Clusters
Learning disabilities rarely travel alone. When a student has a breakdown in one area of information processing, adjacent areas are often affected.
- Dyslexia and Dysgraphia: Dyslexia frequently co-occurs with dysgraphia. The neurological difficulty in phonological processing (reading) often spills over into the motor-orthographic processes required for writing.
- Dyslexia and Dyscalculia: A deficit in working memory and symbolic processing often affects math just as it affects reading. Consequently, dyscalculia frequently co-occurs with dyslexia.
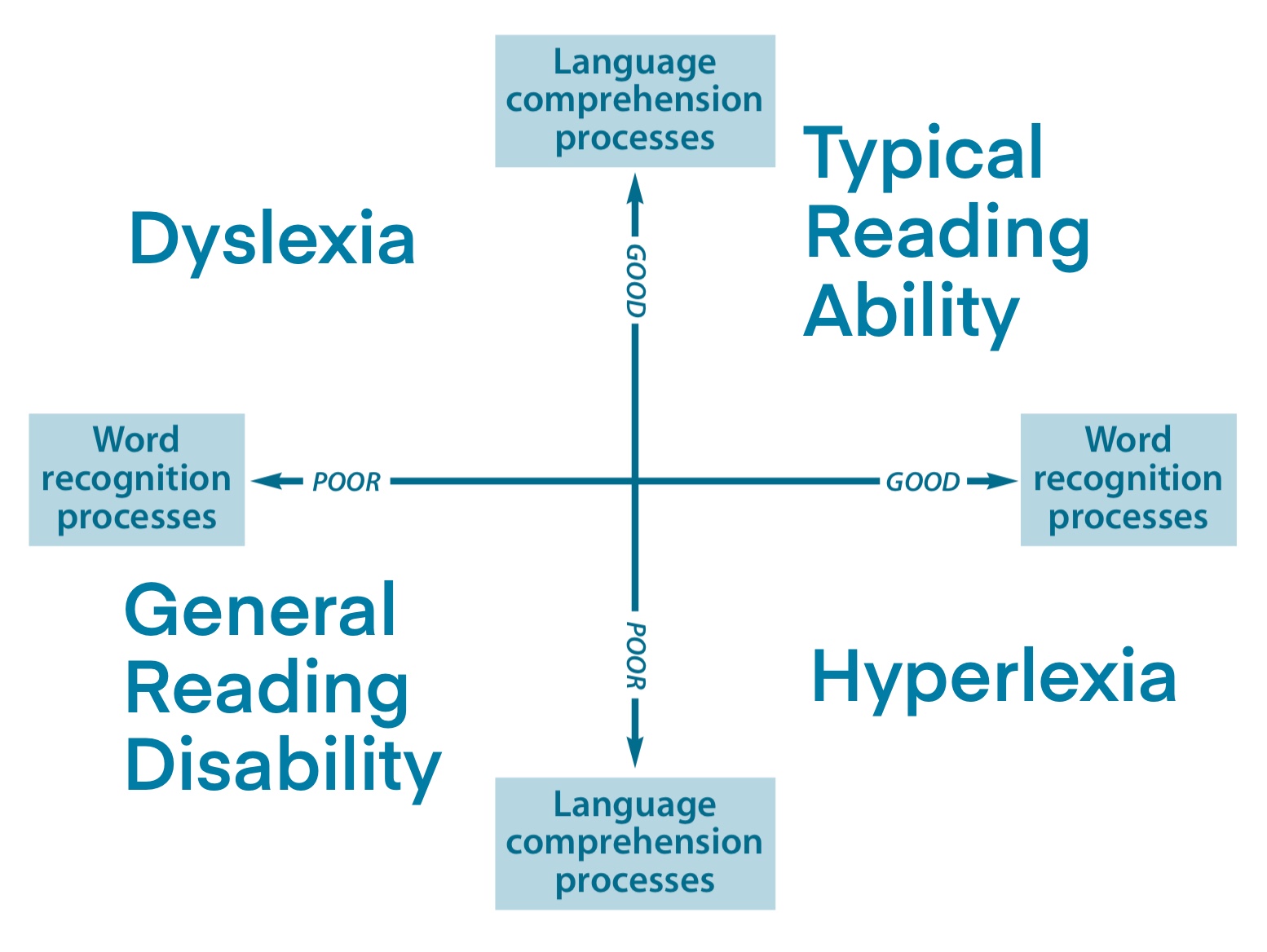
- Reading and Language Overlaps: Specific Learning Disabilities in reading frequently co-occur with expressive language disorders. This is a devastating combination if left untreated, because co-occurring language disorders and reading disabilities severely impair reading comprehension. The student struggles not only to decode the words on the page but also to process the syntax and vocabulary those words represent.
Autism, Intellectual Disabilities, and Medical Complexities
- Autism and Anxiety: The sensory processing difficulties and social-communication barriers inherent in ASD make navigating the world incredibly stressful. As a result, anxiety disorders are highly prevalent in children diagnosed with Autism Spectrum Disorder.
- Neurological Overlaps: Electrical misfires in the brain often accompany developmental differences. Epilepsy frequently co-occurs with Autism Spectrum Disorder, and similarly, epilepsy is a common co-occurring medical condition in individuals with Intellectual Disabilities.
%2C_dystonia%2C_epilepsy_and_schizophrenia.svg)
- Motor and Speech: Brain pathways for physical coordination and speech articulation are tightly linked. Thus, developmental coordination disorders frequently co-occur with Speech and Language Impairments.
- Tourette Syndrome and OCD: Beyond ADHD, a high percentage of individuals with Tourette syndrome also experience Obsessive-Compulsive Disorder. The neurological mechanisms driving physical tics are closely related to the mechanisms driving obsessive, looping thoughts.
| Primary Condition | Highly Common Co-Occurring Condition | Educational Impact |
|---|---|---|
| ADHD | Specific Learning Disability (SLD) | Working memory deficits destroy decoding and comprehension efforts. |
| Dyslexia | Dysgraphia / Dyscalculia | Severe struggles across all core academic outputs (reading, writing, math). |
| Autism (ASD) | Anxiety / Epilepsy | High risk of sensory/emotional overload; medical emergencies (seizures). |
| Tourette Syndrome | Obsessive-Compulsive Disorder (OCD) | Intense anxiety and looping behaviors interrupt academic focus. |
Perhaps the most vital concept for an aspiring teacher to grasp is the causal relationship between unaccommodated academic deficits and downstream behavioral or emotional collapse.
The Secondary Emotional Toll
When a student has a learning disability, the primary deficit is academic. The secondary deficit, however, is deeply emotional. Repeated academic failures related to an unaccommodated learning disability significantly increase the risk of secondary anxiety and depression. Year after year of trying your hardest only to fail in front of your peers breaks a child's psychological resilience. Therefore, it is no surprise that depression is a common secondary emotional condition for students with chronic learning disabilities.
The Behavioral Mirage
Behavior is communication. But when a student has overlapping disabilities, teachers often misinterpret the message.
The presence of a severe behavioral disorder alongside a learning disability often leads teachers to overlook the underlying academic deficit. Imagine a sixth-grader who flips his desk and storms out of the room every day during reading time. The teacher sees "defiance" and writes a behavioral plan to punish the outburst. But the teacher missed the fact that the student is reading at a second-grade level, and flipping the desk is his mechanism for escaping the profound humiliation of being asked to read aloud.
This leads to an absolute rule in special education: Addressing a behavioral challenge without remediating a co-occurring learning disability usually results in failed behavioral interventions. You cannot punish a child into reading better. If the behavior is an escape from academic frustration, the only effective behavioral intervention is academic remediation.
Similarly, unchecked behavioral disorders mutate over time. Conduct Disorder often develops in adolescents who have a history of untreated Oppositional Defiant Disorder. Early, holistic intervention is critical to stop this developmental cascade.
Conducting the Functional Behavioral Assessment (FBA)
When a student with complex, multiple disabilities exhibits interfering behavior, the school must conduct a Functional Behavioral Assessment. But standard FBA procedures must be adapted for complexity.
Functional behavioral assessments for students with multiple disabilities must account for the impact of both cognitive deficits and sensory impairments on behavior. If a student with profound intellectual disability and a visual impairment is lashing out, the FBA cannot merely observe the antecedents and consequences in the classroom environment. The assessor must ask: Is the student in physical pain? Is the lighting in the room causing sensory agony that they cannot verbally communicate due to their cognitive deficits?
When you sit for your exam—and more importantly, when you stand before your classroom—remember that human beings are complex systems. When you see ADHD, look for the SLD. When you see severe behavior, look for the hidden academic deficit driving it. When you evaluate a child with Autism, shine a light into the shadows to ensure an anxiety disorder isn't hiding there. By understanding the intricate web of co-occurring conditions, you transform yourself from a mere manager of symptoms into an architect of genuine student success.